What you’ll learn in this article…
- Roughly 79 percent of U.S. adults report concern about gun violence, per a 2024 Ad Council Research Institute poll.
- More than one in three adults now avoid concerts, malls, or houses of worship because they fear a mass shooting.
- Repeated media exposure after high-profile shootings can directly elevate anxiety, even in people with no personal connection to the event.
- Licensed counselors use evidence-based approaches like CPT and prolonged exposure therapy to help communities recover after gun violence.
Nearly four in five American adults report concern about gun violence, and more than one in three now avoid public spaces such as movie theaters, concerts, and shopping malls because of mass-shooting fear. Unlike other public-safety worries that spike and then fade, gun violence anxiety has become a persistent background hum in millions of lives, tracked by national mental-health organizations and pollsters alike.
The anxiety is not distributed evenly. Black and Hispanic adults report higher levels of fear than white adults, young adults worry more than older generations, and residents of high-violence cities feel the burden most acutely. Media coverage after high-profile shootings can sharpen the anxiety for weeks, even in low-incidence regions.
Clinical thresholds matter. Normal concern becomes a treatment target when it triggers avoidance, sleep disruption, or hypervigilance that persists long after an immediate threat has passed.
How Widespread Is Gun Violence Anxiety in the U.S.?
Nearly four in five U.S. adults (79 percent, according to a 2024 Ad Council Research Institute poll) say they are concerned about gun violence in America.1 That figure places gun violence among the most broadly felt anxieties in the country, cutting across political affiliation, income, and geography.
A Fear That Has Grown Over Time
Putting that number in historical context matters. Gallup data show that personal safety fears reached a three-decade high in the early 2020s, driven partly by a surge in high-profile mass shootings and sustained media attention.2 While a 2025 Gallup-tracked analysis suggests crime fears have eased somewhat, with about 49 percent of adults perceiving crime as a serious national problem, the underlying anxiety about gun violence specifically has remained stubbornly elevated compared to pre-pandemic baselines.3 The modest easing of general crime concern does not appear to have pulled gun violence worry down at the same rate, which suggests the two fears operate somewhat independently in the public mind.
For reference, Gallup's 2023 personal safety data found that 40 percent of U.S. adults reported being afraid to walk alone at night in their own neighborhood, a figure that had climbed sharply from earlier in the prior decade.2 Fear of gun violence is likely a meaningful contributor to that number, though it is not the only driver.
Adults Versus Younger Americans
Anxiety about gun violence is not distributed evenly across age groups. Survey data consistently show that parents and younger adults carry a heavier psychological load than older cohorts, in part because schools and public spaces feel more personally relevant to them. The 2024 Ad Council data found that 75 percent of respondents believe children and teens are the population most affected by gun violence, a perception that likely amplifies parental anxiety considerably.1 Teens themselves report significant stress around school safety, though precise prevalence figures from adolescent-specific studies are harder to pin down without overstating confidence in any single data point.
Gun Violence Fear in the Broader Landscape of American Anxiety
Compared to other major fears, gun violence ranks high. Concerns about terrorism, natural disasters, and general crime are also common, but the 79 percent concern rate for gun violence suggests it has moved from a niche worry into something closer to a background condition of American life. Notably, only about 26 percent of adults in the same 2024 poll were aware that guns are a leading cause of death among children, which means a large share of people feel anxious about the issue without having a full picture of its statistical scope.1 That gap between emotional response and factual framing is worth keeping in mind when thinking about how gun violence anxiety develops and persists.
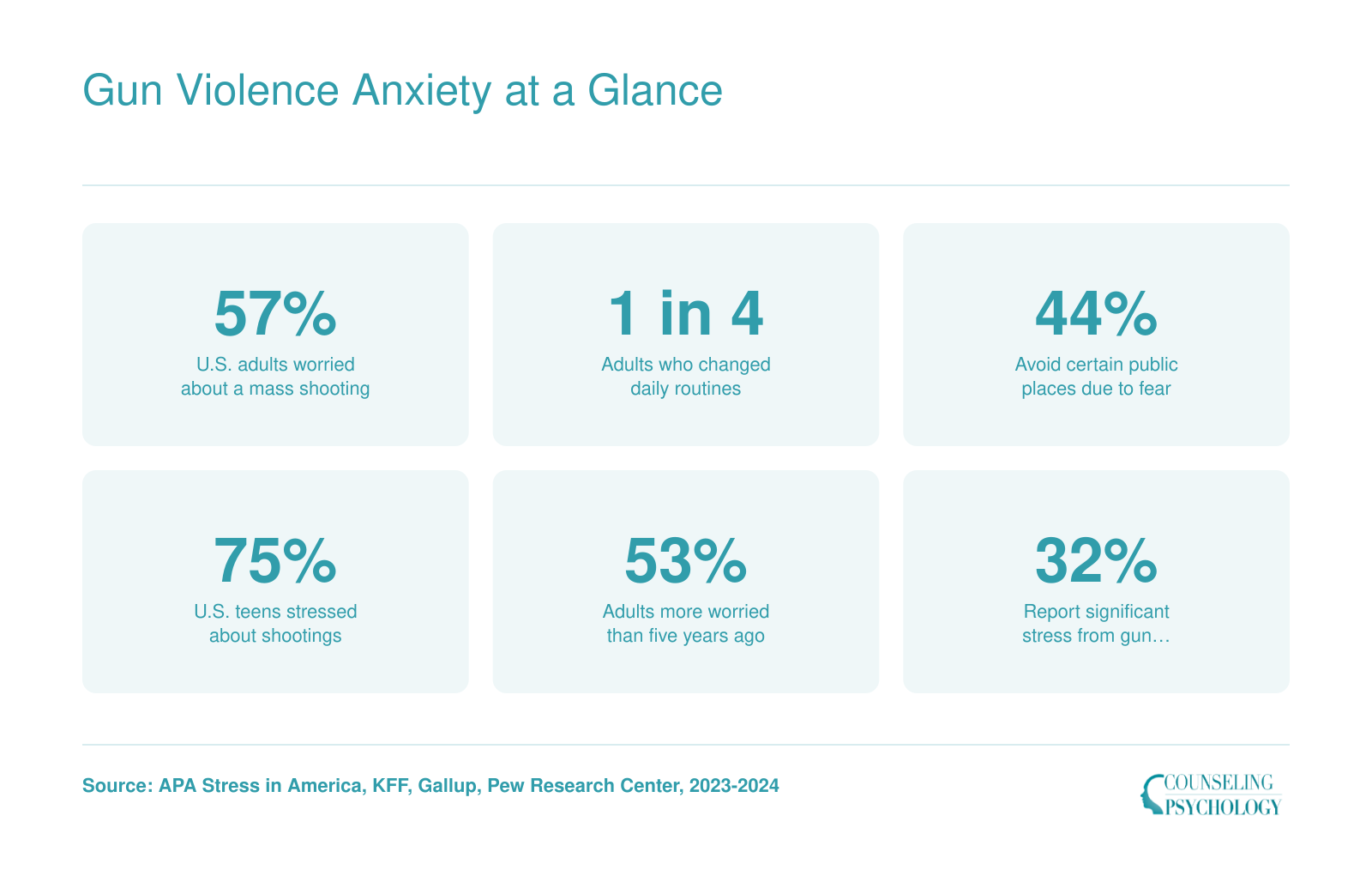
Gun Violence Anxiety at a Glance
National surveys consistently show that fear of gun violence shapes how millions of Americans think, feel, and move through public life. These figures capture the scale of that anxiety across the population.
Gun Violence Anxiety by Demographics: Age, Race, Gender, and Region
How does gun violence anxiety differ by race, gender, age, and where you live?
Race and Ethnicity: Disparities in Exposure and Fear
People of color often report different anxieties about gun violence compared to white Americans, largely shaped by proximity to community violence. Black and Hispanic populations tend to live in areas with higher rates of gun-related incidents, meaning their fears are frequently anchored in personal safety during daily activities. Surveys from the Pew Research Center indicate that nonwhite adults are more likely to view gun violence as a major problem and to express worry about becoming a victim. While 49 percent of all U.S. adults in 2024 identified gun violence as a major concern, the number is typically higher among Black respondents in urban settings where gun homicides are more prevalent.1 Among white Americans, anxiety often skews toward high-profile mass shootings rather than routine neighborhood violence, reflecting different lived realities. These disparities also highlight gaps in access to culturally responsive care, an issue explored in research on BIPOC therapists and their availability across the country.
Gender Gap: Women Report Higher Anxiety
Consistent across multiple polls, women report significantly greater anxiety about gun violence than men. APA Stress in America surveys repeatedly show that women are more likely to cite mass shootings as a source of stress, and KFF polling finds a double-digit gap in worry levels. The gender divide appears in both general fear and in specific concerns about school shootings, which may intersect with caregiving roles. Men are not only less likely to express anxiety, but research suggests they may underreport fear due to social norms around male emotional expression. The result is that mental health professionals must often work harder to identify underlying distress in male patients who have been affected by gun violence exposure.
The Prior-Trauma Multiplier
A personal history with gun violence dramatically amplifies anxiety. People who have witnessed a shooting, lost a family member to gun violence, or survived an incident themselves report symptoms that are several times more severe than those with only media-based exposure. Studies in the American Journal of Preventive Medicine indicate that direct victims often meet criteria for post-traumatic stress and can experience an odds ratio of two to three times the general population for severe anxiety. Even secondhand exposure, such as knowing a victim or living in a neighborhood with frequent gunfire, multiplies the risk. This multiplier effect underscores why clinicians always screen for trauma history when patients present with gun-related fear.
Regional and Urban-Rural Contrasts
Where someone lives shapes how gun violence anxiety manifests. Urban residents frequently cite fear of street-level violence and home invasions, while those in suburban and rural areas are more likely to name school shootings or random mass casualty events as their primary fear. These are not separate psychological conditions but different expressions of the same underlying concern about safety. Worry about school shootings is not confined to any one region: 59 percent of public K-12 teachers nationwide reported being worried about a shooting at their school in the 2022-2023 school year, a statistic that cuts across geography.2 This dual pattern means that counselors pursuing careers in counseling must tailor coping strategies to the specific threat landscape each patient perceives.
Questions to Ask Yourself
The States and Cities Where Gun Violence Concern Is Highest
Gun violence concern is the level of worry, fear, or anxiety residents report about being shot or witnessing gun violence in their community. It tracks loosely, but not perfectly, with actual gun death rates: a state with a high rate of firearm deaths usually produces more anxious residents, but media exposure, recent local incidents, and policy debates can push concern higher even in places with relatively low statistical risk.
States with the Highest Firearm Death Rates
CDC WONDER's age-adjusted firearm death rates are the cleanest starting point for understanding where physical risk, and by extension chronic worry, runs highest. In 2023, Alabama recorded 23.7 firearm deaths per 100,000 residents, and Alaska reached 24.4 per 100,000, both well above the national average.1 At the other end, Hawaii reported just 3.7 deaths per 100,000, one of the lowest rates in the country.1 Mississippi, Louisiana, Wyoming, and New Mexico also consistently sit near the top of the rate rankings, and Gallup's state-level safety polling tends to mirror that pattern.
Policy Environment and Public Worry
Gun law strength does not map onto concern in a one-to-one way, but it shapes the conversation residents hear daily. The Everytown 2026 State Gun Law Rankings place California at #1 for the strength of its firearm laws, while Florida ranks 23rd.23 The Giffords Annual Gun Law Scorecard reaches similar conclusions using a slightly different methodology. Residents in states with weaker laws frequently report higher baseline worry in academic surveys, including those published by the Harvard Injury Control Research Center.
Finding City-Level Data
Metro-level numbers are harder to pin down. A few practical routes:
- Federal crime data: The FBI's Uniform Crime Reporting program and the Bureau of Justice Statistics' annual victimization surveys publish violent and firearm crime rates for major metros.
- Local public health reports: County and city health departments often run community fear-of-crime modules and post results on open data portals.
- Advocacy scorecards: Everytown for Gun Safety publishes city-level scorecards that combine policy and outcome measures.
- Direct outreach: For a specific city, the police department's community survey office and local news polling desks can share commissioned data that never makes it into national datasets.
Triangulating two or three of these sources gives a more honest picture than any single number.
How Media Coverage Amplifies Gun Violence Fear
What does the research actually show about the link between media exposure to gun violence and rising anxiety levels? A growing body of evidence suggests that the way we consume news, especially after high-profile shootings, can directly shape our mental health. While staying informed feels responsible, the saturation of graphic images and round-the-clock updates may be fueling a cycle of fear that extends far beyond the immediate events.
The Research on Media Exposure and Anxiety
A landmark study by Holman and colleagues, published in the Proceedings of the National Academy of Sciences, examined responses to the Boston Marathon bombing. It found that people who consumed six or more hours of daily media coverage in the week following the attack reported acute stress symptoms at rates three times higher than those who were directly at the bomb site but had minimal media exposure. This dose-response relationship highlights that repeated exposure to violent imagery and distressing narratives can retraumatize viewers, even those with no personal connection to the event.
Other work, such as Pfefferbaum's research on terrorism and media, confirms that graphic news coverage correlates with elevated anxiety and post-traumatic stress symptoms in both adults and children. A 2019 analysis in JAMA Network Open noted that frequent exposure to news about mass shootings was associated with a measurable increase in generalized anxiety, particularly among populations who already felt vulnerable. Clinicians refer to this phenomenon as "distal trauma," where secondhand exposure through screens can produce genuine psychological distress. Understanding how group-level perceptions of threat develop is a core concern in the field; researchers trained as social psychologists have contributed significantly to this body of work.
Why Media Coverage Hits Harder Now
Today's media landscape amplifies these effects. Social media algorithms serve repetitive, emotionally charged content, while push notifications deliver breaking news instantly. The sheer volume and velocity of coverage can make gun violence feel ubiquitous, even when statistical risk remains low. Research suggests that the human brain processes vivid, fear-inducing images more deeply than abstract statistics, leading to an overestimation of threat. This negativity bias, exploited by 24/7 news cycles, can make anxiety feel inescapable.
Guidelines from Leading Health Organizations
The American Psychological Association (APA) recommends intentional media consumption limits, particularly after mass violence. Their guidance includes designating specific times to check news, avoiding exposure right before bed, and using trusted, fact-based sources rather than relying on social media feeds. The Substance Abuse and Mental Health Services Administration (SAMHSA) similarly stresses the importance of "media dieting" during periods of heightened stress, advising people to monitor their emotional reactions and step away when coverage triggers anxiety or hopelessness.
The CDC's Violence Prevention resources add practical steps for families: talk openly with children about their fears, maintain routines, and model healthy coping. Parents should preview news content before sharing it with minors and emphasize the helpers and community resilience stories that often get less airtime. Professionals interested in supporting survivors of interpersonal violence may also consider learning how to become a domestic violence counselor.
Practical Ways to Dial Down Media-Induced Anxiety
- Set a time limit: Use a timer for news consumption and stick to it, even when updates are still unfolding.
- Curate your feed: Follow outlets that report facts without sensationalism and mute accounts that share graphic footage without warning.
- Balance with positive action: After reading distressing news, channel anxiety into productive steps like supporting violence prevention organizations or attending a community safety meeting.
- Check your body: Notice physical signs of stress (racing heart, shallow breathing) and use grounding techniques before returning to coverage.
Media will always report on violent events, but you control how and how much you engage. By recognizing the link between media consumption and anxiety, you can protect your mental health while staying informed.
Related Articles
When Fear Becomes a Clinical Problem: Symptoms and Screening
Worry about gun violence is a normal human response to real danger, but that worry crosses into clinical territory when it persists long after the immediate threat has passed and begins to interfere with daily functioning. Understanding the distinction between temporary heightened vigilance and a diagnosable anxiety disorder can help you recognize when professional support is warranted.
The Line Between Normal Worry and Clinical Anxiety
After hearing news of a mass shooting or violent incident, most people experience a temporary spike in alertness. You might find yourself scanning exits at a movie theater, checking news updates compulsively, or feeling on edge in crowded spaces. For most adults, these reactions fade within two to four weeks as the acute stress response naturally resolves.
However, the DSM-5-TR establishes clear duration thresholds that separate transient distress from diagnosable conditions. Acute Stress Disorder applies when significant symptoms emerge immediately after trauma but resolve within one month.1 If symptoms persist beyond that one-month mark, a PTSD evaluation becomes appropriate, since the DSM-5-TR sets a minimum symptom duration of one month for that diagnosis.1 Generalized Anxiety Disorder requires symptoms to be present for at least six months and to cause clinically significant distress or impairment across multiple life domains.5
Red-Flag Symptoms That Warrant Attention
Certain symptom patterns signal that fear has moved beyond adaptive caution:
- Persistent intrusive thoughts: Unwanted, repeated mental images of violence or harm that intrude throughout the day, even when you are trying to focus on other tasks.
- Avoidance lasting more than a month: Refusing to enter public spaces such as schools, malls, theaters, or places of worship specifically because of shooting fears, and maintaining that avoidance for longer than four weeks.
- Hypervigilance that disrupts functioning: Constantly scanning for threats to the point that it interferes with concentration at work, strains relationships, or leaves you exhausted.
- Sleep disruption: Difficulty falling asleep, staying asleep, or experiencing nightmares related to violence.
- Emotional numbing: Feeling detached from loved ones, losing interest in activities you previously enjoyed, or experiencing a persistent sense of unreality.
Research on mass violence exposure indicates that direct trauma survivors typically show symptom improvement within one to three months with appropriate support.1 When symptoms remain stable or worsen beyond this window, clinical intervention becomes increasingly important. Professionals such as crisis counselors and suicide prevention specialists are trained to address exactly this kind of persistent distress.
Validated Screening Tools You Can Use
Two widely accepted instruments can help you gauge whether your symptoms have reached a level that merits professional evaluation.
The GAD-7 is a seven-item questionnaire that screens for generalized anxiety.2 Each item is scored from 0 to 3, yielding a total score between 0 and 21. Scores of 0 to 4 indicate minimal anxiety, 5 to 9 suggest mild anxiety, 10 to 14 reflect moderate anxiety, and 15 to 21 signal severe anxiety.3 A score of 10 or higher is the standard threshold at which further clinical follow-up is recommended.2 The GAD-7 is free, takes about two minutes to complete, and is available through the Anxiety and Depression Association of America and numerous healthcare provider websites.
The PCL-5 is a 20-item self-report measure designed specifically for PTSD. Each item is scored 0 to 4, producing a total between 0 and 80. A score in the 31 to 33 range is commonly used as the cutoff for probable PTSD, though formal diagnosis requires a clinical interview.4 Like the GAD-7, the PCL-5 is free and publicly accessible.
Neither tool replaces a professional evaluation, but both offer a starting point for understanding whether your symptoms fall within typical ranges or suggest a need for further assessment.
When to Seek Professional Evaluation
If your symptoms have persisted for more than one month after a triggering event, or if you score at or above the clinical thresholds on the GAD-7 or PCL-5, scheduling an appointment with a licensed mental health professional is a reasonable next step. Early intervention tends to produce better outcomes, and effective treatments exist for both generalized anxiety and PTSD.
More than one in three U.S. adults avoid concerts, movie theaters, houses of worship, or shopping malls because they fear a mass shooting, recent surveys show. Workplace anxiety is rising too: active-shooter drills are now standard in many organizations, yet some employees find them more anxiety-provoking than reassuring.
Evidence-Based Coping Strategies for Gun Violence Anxiety
What actually works to reduce anxiety about gun violence, and which approach should you try first? The honest answer from the research literature is that no single intervention dominates. Clinicians from the American Psychological Association and SAMHSA consistently recommend matching the strategy to the severity of distress, then layering approaches as needed.
Comparing the Five Main Approaches
Here is how the most studied options stack up:
- Trauma-Focused CBT: Includes psychoeducation, exposure work (both imaginal and in vivo), cognitive restructuring, and anxiety-management skills. Best for adults with clinically significant symptoms such as PTSD, panic, or generalized anxiety. Evidence level is strong (Level I), with decades of randomized controlled trials behind it. Requires a licensed therapist trained in trauma protocols.1
- Psychological First Aid (PFA): A brief, structured framework focused on promoting safety, calming, self-efficacy, social connection, and hope in the hours and days after a violent event. Best for acute post-event stabilization, not chronic worry. Evidence is informed by clinical consensus but has limited RCT support (Level II to III). Can be delivered by trained paraprofessionals and community responders, not just licensed clinicians.2
- Skills for Psychological Recovery (SPR): A multi-session resilience program covering problem-solving, helpful thinking, and managing reactions. Best for subclinical distress and post-disaster recovery when symptoms persist beyond the acute phase. Moderate evidence (Level II). Typically delivered by trained providers but uses a structured workbook format.2
- Media Literacy Interventions: Teach critical evaluation of news sources, base-rate reasoning (the actual statistical risk versus perceived risk), and intentional limits on doom-scrolling. Best for chronic ambient anxiety driven by saturation coverage. Emerging to moderate evidence (Level II to III). Largely self-directed, which makes it widely accessible.3
- Mindfulness-Based Stress Reduction (MBSR): An 8-week group program teaching mindfulness of breath and body, and observing worry without engaging it. Best as an adjunct to CBT or for self-management when threat feels ongoing. Moderate evidence (Level II). Available through community classes, apps, and clinical programs.4
Why Combining Strategies Works Better
Reviews of mass-violence mental health responses, including the APA's Gun Violence: Prediction, Prevention, and Policy report and NIH analyses of mass shooting impacts4, consistently endorse stepped-care and multi-modal approaches. A typical recommended sequence starts with PFA in the immediate aftermath, moves to media-use limits and mindfulness for ongoing ambient stress, and escalates to trauma-focused CBT if symptoms cross into clinical territory. Those drawn to this kind of work may consider becoming a crisis intervention specialist, a role that directly applies PFA and stepped-care models. Peer support groups can run alongside any of these strategies. Relying on one approach alone, especially for chronic anxiety with both physiological and cognitive components, leaves too much of the picture untreated.
How Counselors and Psychologists Help Communities Heal
After a mass shooting, communities face a painful tension: the urge to restore physical spaces and daily routines clashes with the need for a slower, more deliberate process of psychological healing. Licensed counselors and psychologists bridge that gap, bringing both immediate relief and long-term recovery strategies to survivors, families, and neighborhoods.
Crisis Response and Community Debriefing
In the hours and days following a mass violence event, mental health professionals deploy as part of crisis response teams. They provide psychological first aid at Family Assistance Centers, help survivors process acute trauma, and lead community debriefing sessions that create a shared space for grief and resilience.1 These interventions are deliberately brief, often lasting 60 days through the Immediate Services Program, to stabilize individuals without overwhelming them.
Long-Term Trauma Therapy and School-Based Interventions
Recovery extends far beyond the initial crisis. Clinical psychologists and counselors offer evidence-based trauma therapies like trauma-focused cognitive behavioral therapy (TF-CBT) and eye movement desensitization and reprocessing (EMDR) to those with persistent distress. In schools, mental health teams screen students for anxiety and depression, run small-group interventions, and train teachers to recognize signs of delayed trauma. Professionals drawn to this work in educational settings may also consider childhood trauma counseling as a specialized career path. This layered approach addresses both individual pain and the collective wounds that linger after gun violence.
Specialized Training Pathways
Professionals who do this work often pursue advanced certifications. Trauma-focused CBT certification prepares counselors to work with children and adolescents, while EMDR training equips psychologists to reprocess traumatic memories. Crisis counseling credentials, such as those offered through national counseling boards, ensure practitioners can respond effectively under disaster conditions. For students considering mental health careers, these pathways offer a direct route into one of the field's most urgent areas of need.
Growing Demand and Career Outlook
The need for trauma-informed mental health services is accelerating. According to national BLS projections, employment of mental health counselors is expected to grow 19% from 2023 to 2033, much faster than average, while psychologist roles are projected to increase 7%. Gun violence is one driver of this demand, but the broad push for accessible mental health care in schools, workplaces, and communities ensures that career prospects remain strong. Students interested in salary benchmarks can explore data on counselor salary by degree and specialty.
SAMHSA's Crisis Counseling Program as a Model
The FEMA-funded Crisis Counseling Assistance and Training Program (CCP), authorized under the Robert T. Stafford Disaster Relief and Emergency Assistance Act, is a cornerstone of federal disaster response.1 Activated after a Presidential major disaster declaration that includes Individual Assistance, the CCP deploys licensed professionals and trained paraprofessionals to provide community mental health counselor services through structured outreach. The 60-day Immediate Services Program often transitions into a nine-month Regular Services Program, offering ongoing individual crisis counseling in homes, schools, and community centers. This model has been used after numerous mass shootings, demonstrating how coordinated, grant-supported efforts can help communities move from shock to sustainable recovery.
Resources and Next Steps
If gun violence anxiety is affecting your daily life or the life of someone you care about, practical help is available right now. Below are answers to the most common questions about accessing support, screening tools, and professional care.