What you’ll learn in this article…
- Over 137 million Americans live in Mental Health Professional Shortage Areas, meeting only 27% of need.
- Hawaii's Act 93 permits pre-licensed therapists to bill insurance, reducing a $8,400 average supervision cost.
- 75% of Hawaii's counseling grad students are local, yet only 33% remain to practice after licensure.
- Telehealth now permanently expands access, but cannot fully close the provider gap.
A single state policy experiment in Hawaii is testing whether licensing reform can slow the mental health workforce exodus. On June 2, 2026, Hawaii opened applications for provisional associate licenses allowing pre-licensed therapists to bill insurance while completing supervised hours.1 The move addresses a brutal reality: 137 million Americans live in shortage areas, and therapy demand grew 34% in five years.
The crisis is driven by costly supervision mandates, insurance reimbursement shortfalls, and chronic attrition. In Hawaii, for every three locally trained therapists, only one remains to practice.1
The Scope of the Mental Health Provider Shortage in 2026
The mental health workforce shortage in 2026 has left over 137 million Americans living in areas with inadequate access to care. As of December 2025, 6,807 geographic areas across the United States qualified as Health Professional Shortage Areas (HPSAs) for mental health, meaning the provider-to-population ratios fall below federal thresholds. With only 27 percent of the need met1, the gap between demand and available clinicians continues to widen, forcing communities into a silent crisis of untreated mental illness.
A Nationwide Crisis in Numbers
Federal definitions provide a stark lens. A region earns a mental health HPSA designation if it exceeds 30,000 people per psychiatrist or 9,000 per core mental health provider, a category that includes clinical psychologists, licensed clinical social workers, psychiatric nurse practitioners, and marriage and family therapists.2 Across all designated shortage areas, an estimated 6,800 additional practitioners are required just to meet minimum targets.1 This shortage does not affect all Americans equally. Rural and frontier counties, tribal lands, and low-income urban neighborhoods bear the heaviest burden of the rural mental health provider shortage, often lacking even a single specialized provider.
Shortages Across Provider Types
The maldistribution cuts across every professional discipline. Psychiatrists are in critically short supply, with some states reporting fewer than one child psychiatrist per 10,000 children. Psychologists and clinical social workers, who perform the bulk of therapy and assessment, are similarly strained, particularly those trained in trauma, substance use, or geriatrics. Marriage and family therapists and psychiatric nurse practitioners, though essential, remain unevenly distributed, concentrating in better-resourced metro areas while local clinics in underserved zones struggle to recruit.
Geographic Disparities: The Hardest-Hit Regions
California illustrates the scale: 627 designated shortage areas covering over 11.5 million residents, with only 23 percent of the provider need met.1 Florida mirrors the challenge with 239 shortage areas and nearly 10 million affected people, meeting just 25 percent of demand.1 Entire states are not immune. Hawaii, for example, is classified as a statewide Mental Health Professional Shortage Area. The tropical image masks a reality where island geography, cost of living, and licensing barriers create a near-perfect storm, leaving residents months away from a first appointment.
The Ripple Effect: Wait Times and Access
In the hardest-hit regions, wait times for therapy stretch to six weeks or longer; for child and adolescent specialists, teen therapy wait times can exceed three months. Emergency departments become the default source of care, and treatable conditions escalate. The growing bottleneck means that even insured patients often cannot find a practitioner accepting new clients, pushing families to drop out of care entirely. Without robust policy intervention, these gaps threaten to deepen as burnout and retirement thin the existing workforce further.
The Shortage in One Number: 137 Million Americans
As of 2025, approximately 40% of the U.S. population resides in areas federally designated as having a shortage of mental health professionals. This staggering figure underscores the urgency of addressing workforce gaps across the country.

Did you know that over 137 million people in the United States live in federally designated mental health professional shortage areas? According to the Kaiser Family Foundation, this staggering number highlights the vast gap in access to care, leaving millions without timely support.
Policy Changes That Are Addressing the Shortage
For aspiring therapists, the path to licensure often pits financial survival against professional development: too many graduates complete their training only to face a wall of unpaid or poorly compensated supervised hours that can delay or derail their careers. Across the country, state and federal policymakers are finally acknowledging that the mental health workforce shortage reflects a pipeline that leaks talent at the very stages where support is most needed. A wave of legislative and regulatory reforms is beginning to reshape that landscape, targeting the licensing bottlenecks, geographic barriers, and economic disincentives that drive providers out of the field or away from underserved communities.
State-Level Licensure Reforms: Closing the Training Gap
A growing number of states are rethinking the post-degree supervision period, which has long been a financial strain for pre-licensed clinicians. Hawaii’s Act 93, signed in 2024 and implemented in mid-2026, offers a case in point. The law creates provisional associate-level licenses for marriage and family therapists, mental health counselors, and psychologists in training. For the first time, those accruing the required 1,000 to 3,000 supervised hours, typically over two years or more, can bill insurance directly, a shift tied to how insurance changes affect mental health counselors, rather than working for free or paying thousands out of pocket. Before this change, roughly 44% of pre-licensed therapists in Hawaii reported average supervision costs of $8,400, a burden that contributed to a brain drain: while 75% of graduate students identified as local, only 33% of surveyed graduates remained in the state.1
Hawaii is not alone. Across the U.S., similar associate licensure bills are percolating, often driven by coalitions of professional associations, universities, and workforce advocates. To track these developments, prospective counselors and psychologists should monitor their state legislature’s website or the policy pages of organizations like the American Psychological Association Practice Directorate, the National Association of Social Workers, and the American Counseling Association. Many bills include provisional billing language, streamlined supervision ratios, or temporary permits that let graduates begin serving clients sooner. Keeping an eye on licensing board rulemaking sessions can catch subtle shifts, such as reduced face-to-face supervision requirements or expanded telehealth allowances, that never make headlines but directly affect thousands of trainees.
Interstate Compacts: Streamlining Mobility
While state-level reforms ease entry, interstate compacts are dismantling the financial and logistical barriers that keep licensed providers tethered to one location. PSYPACT, the Psychology Interjurisdictional Compact, now includes a substantial bloc of states, allowing licensed psychologists to practice across state lines via telepsychology or temporary in-person authorization without obtaining a full new license. The Counseling Compact is similarly expanding mobility for licensed professional counselors. For clinicians in shortage areas, these agreements can mean the difference between an isolated practice and a balanced panel of clients from multiple regions. As more states join and implementation guidance matures, compact participation is becoming a factor in career planning for graduate students who may eventually relocate or serve rural populations.
Federal Initiatives: Loan Repayment and Workforce Monitoring
Federal programs provide another layer of incentive for staying in underserved areas. The Health Resources and Services Administration’s National Health Service Corps offers loan repayment for licensed mental health providers who commit to working in designated shortage facilities. While demand far exceeds funding, the program’s existence signals federal recognition of the problem. The Bureau of Labor Statistics continues to project growth rates for mental health occupations well above the national average, reinforcing the idea that policy interventions must keep pace with demand.
For anyone navigating this shifting policy environment, the best strategy is active engagement. Check your state’s professional licensing board newsletters, join association advocacy lists, and frequently revisit the HRSA workforce pages. The rules are changing fast, and the difference between struggling in silence and stepping into a supported career often hinges on knowing which doors have just been unlocked.
A 2022 Hawaii survey found that 44% of pre-licensed therapists paid an average of $8,400 for mandatory supervision while working for free or minimal pay, a cost that contributed to the state's therapist exodus. With Act 93, these clinicians can now bill insurance during their supervised hours, directly reducing the financial strain that pushed many out of the field.
How Insurance Barriers Exacerbate Provider Access
Insurance barriers to mental health care are the practical hurdles that stop people from using their health coverage to actually see a therapist: ghost networks, reimbursement shortfalls, and parity rules that exist on paper but not in practice. Even when a person has insurance that supposedly includes mental health benefits, finding an available, in-network provider often becomes a demoralizing scavenger hunt. These systemic cracks don't just inconvenience patients; they directly shrink the pool of clinicians willing to accept insurance, deepening the access crisis.
The Problem of Ghost Networks and Outdated Directories
- Ghost networks: Many insurance provider directories list therapists who are not accepting new patients, have moved, or never accepted the plan in the first place.
- Long wait times: Even when a listed provider is real, wait times for an initial appointment can stretch weeks or months; New York State now mandates that health plans ensure behavioral health appointments within 10 business days.2
These directory failures inflate out-of-network usage: psychologists are 10.6 times more likely than specialty physicians to be seen on an out-of-network basis, and 8 times more likely than primary care physicians.1 Patients pay more, access drops.
Reimbursement Gaps That Push Therapists Out of Network
A core reason clinicians drop or never join insurance panels is money. Behavioral health office visits are reimbursed about 22% less than comparable physical health visits, according to data from 2024.1 For a therapist running a small practice, that gap makes it financially untenable to sustain a full caseload of insured clients. The result: many experienced providers shift to private-pay models, while newly licensed clinicians, already facing supervision costs and student debt, see no viable path to accepting insurance.
When reimbursement doesn't cover overhead, providers leave networks voluntarily, narrowing the pool further. This mimics a self-reinforcing cycle: lower rates shrink networks, which drives up out-of-network utilization, which then gets cited as evidence that networks are adequate.
Parity on Paper, Not in Practice
The Mental Health Parity and Addiction Equity Act (MHPAEA) requires insurers to cover mental health care on par with physical health. Yet enforcement has been inconsistent. Final federal rules were issued in September 2024 and took effect in January 2025, but in May 2025 the administration announced a non-enforcement policy, essentially pausing compliance requirements.1 Meanwhile, studies show that implementing full parity improves outcomes without raising overall costs,1 yet denial rates for mental health claims remain higher than for medical claims, and state-level compliance is patchy.
A few states have moved ahead: New York's 2025 regulations require health plans to demonstrate adequate behavioral health networks, submit annual access plans, and treat out-of-network mental health visits with in-network cost-sharing.2 But nationally, parity remains an aspiration rather than a reality.
Why This Hurts New Clinicians and Patients Alike
Low reimbursement rates are especially punishing for pre-licensed therapists. In many states, associates must complete 1,000 to 3,000 supervised hours before full licensure, often while paying for supervision and earning little. If insurance panels won't reimburse pre-licensed clinicians at sustainable rates, those associates have to choose between working for free in community clinics or leaving the field entirely. Hawaii's Act 93 directly tackles this by letting associate-level therapists bill insurance during supervision, but such policies remain rare. Until reimbursement adequately values mental health services, the pipeline of providers will keep leaking, and wait lines will keep growing in states with states with highest need for counselors.
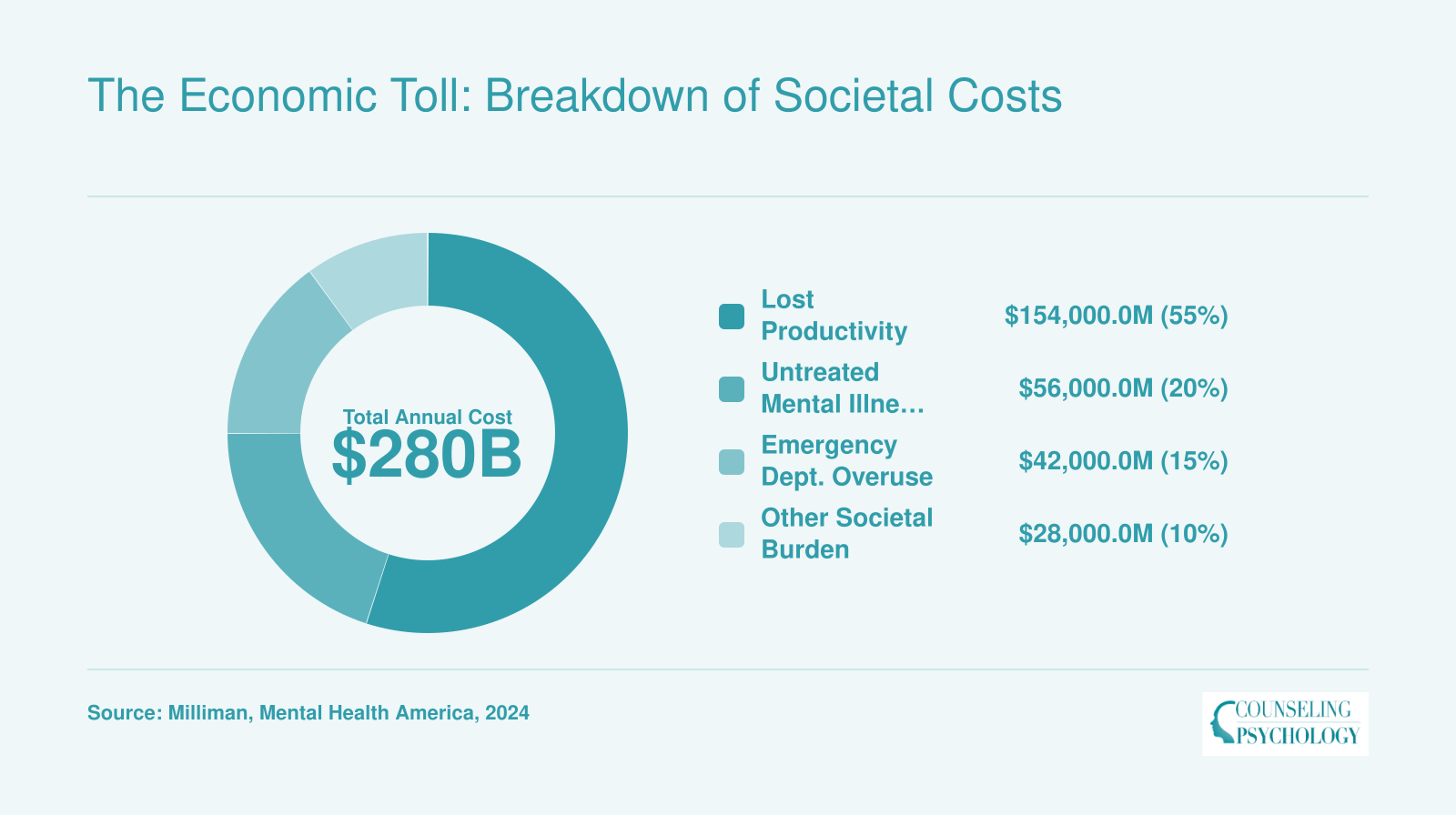
The Economic Toll: Breakdown of Societal Costs
The mental health provider shortage carries a staggering economic price tag. Lost productivity from untreated depression and anxiety accounts for the largest share, while preventable emergency room visits and the downstream costs of unaddressed mental illness add billions more. These figures, extrapolated from Milliman and Mental Health America analyses, reflect a systemic burden that extends far beyond the therapist’s office.
Questions to Ask Yourself
Can Telehealth Bridge the Gap?
Telemental health has moved from a temporary necessity during the pandemic to a permanent fixture of mental health care, yet its ability to meaningfully close the provider shortage remains contested.
The State of Telemental Health Today
National data paint a complex picture of telehealth's role in mental health. In 2026, 12.0% of U.S. adults received outpatient mental health care, but only 3.3% used exclusively telemental health services and 2.6% combined telehealth with in-person visits.1 Counseling or therapy reached 14% of Americans in 2024.2 These figures show that while telehealth expands options, most care still happens in traditional settings. The persistent gap is underscored by the fact that 25% of adults with mental illness reported unmet need in 2022, 20233, and 122 million Americans live in underserved areas.4
Does Telemental Health Work?
Research supports the clinical effectiveness of virtual therapy. A meta-analysis found that telemental health interventions had a moderate effect size of 0.84 for reducing depression, comparable to in-person treatment.5 Patient satisfaction is generally high, and many clinicians now offer hybrid models that blend technology in counseling with in-person sessions. This evidence has encouraged insurers and regulators to maintain pandemic-era flexibilities, but outcomes vary by condition and patient engagement. For individuals in rural regions where providers are scarce, telehealth has dramatically cut wait times. In Hawaii, for instance, a 2022 survey found that 78% of local providers identified mental health counseling as the most critically needed specialty, a gap that virtual sessions can help fill when the local workforce is thin.
Barriers That Limit Reach
Despite its promise, telemental health faces stubborn obstacles. Interstate licensure restrictions prevent many clinicians from treating patients across state lines, fragmenting care even when digital tools would allow seamless connection. Broadband access remains uneven, leaving some rural and low-income communities unable to sustain video sessions. Insurance reimbursement for telehealth services is inconsistent, with some payers imposing lower rates or reimposing in-person requirements. These structural issues mean that telehealth alone cannot fix the shortage; it is one tool among many.
A Partial Fix, Not a Panacea
Telehealth will continue to grow, but workforce shortages, reimbursement politics, and digital divides require parallel policy solutions. Provisional licensing reforms like Hawaii's Act 93, which allows pre-licensed clinicians to bill insurance, address financial hurdles that push graduates out of the field. Telehealth can amplify the impact of those reforms by connecting newly licensed providers with patients in shortage zones, but it cannot replace the need for training pipelines, loan forgiveness programs, and state-level action to boost retention. The gap will narrow only when virtual care is integrated with systemic workforce investments.
Telehealth Effectiveness by the Numbers
Telehealth has transformed mental health care delivery, expanding access and maintaining high satisfaction. Key metrics from 2025 highlight its widespread adoption and effectiveness among patients and providers.

State-By-State Shortage Data and Regional Disparities
Mental Health Professional Shortage Areas (HPSAs) highlight where Americans struggle most to access care. As of December 2025, more than 6,800 designated HPSAs across the U.S. cover over 137 million people, yet only 27.29% of the need is met nationwide.1 The table below ranks states by key shortage indicators, drawing on 2025, 2026 Health Resources and Services Administration (HRSA) data.
Snapshot of Shortage Severity Across States
| State | HPSA Designations | Population in HPSAs | Percent Need Met | HPSA Score (1-25)* |
|---|---|---|---|---|
| United States (total) | 6,807 | 137,133,953 | 27.29% | , |
| California | 627 | 11,542,855 | 23.49% | , |
| Florida | 239 | 9,871,089 | 24.87% | 17.5 |
| Georgia | 92 | 5,065,892 | 45.31% | , |
| District of Columbia | , | , | , | 19.0 |
| Louisiana | , | , | , | 18.0 |
| Kentucky | , | , | , | 17.6 |
| Illinois | , | , | , | 17.3 |
*HPSA scores range from 1-25; higher values indicate greater shortage severity. Scores are not reported for all states.2 Population data reflects residents within federally designated shortage areas.
Interpreting the Disparities
The “Percent Need Met” column tells a stark story: California and Florida satisfy less than a quarter of their mental health workforce requirements, lagging far behind the already low national average. Georgia’s 45.31% looks better by comparison, but nearly 5.1 million Georgians still live in HPSAs. Where HPSA scores are available, such as the District of Columbia (19.0) and Louisiana (18.0), they confirm extreme strain, often driven by a combination of high uninsured rates, deep poverty, or concentration of providers in urban enclaves.
The Rural, Urban Divide
Regional disparities become even more pronounced when examining provider-to-population ratios. While detailed breakdowns for psychiatrists, psychologists, and clinical social workers are not uniformly published at the state level, HRSA data consistently show that rural counties face far greater shortages than metropolitan areas. For example, many rural counties lack even a single psychiatrist or doctoral-level psychologist, forcing residents to travel hours for care. In contrast, urban centers like New York City or Boston may have relatively high provider densities but still contain underserved neighborhoods due to maldistribution and insurance barriers. This urban-rural gap widens the effective shortage: even states with moderate overall numbers often have vast deserts of care outside major cities.
What the Data Doesn’t Show
The raw HPSA figures undercount the true access problem because they measure designated shortage areas, not individual provider availability or insurance acceptance. A county can avoid HPSA designation yet still have waitlists of months if most clinicians do not accept Medicaid or private insurance. Similarly, the data focus on psychiatrists, psychologists, and clinical social workers in certain settings, potentially missing other licensed counselors and marriage and family therapists who deliver crucial care. As policymakers debate funding and licensure reforms, these state-by-state snapshots underscore the uneven impact of the mental health provider shortage , a burden that's particularly acute in states with the highest unmet need for mental health professionals , and the need for targeted solutions that address both raw numbers and geographic distribution.
Seventy-five percent of our graduate students are local, but only 33% of surveyed graduates still practice in Hawaii.
How to Find a Therapist in a Shortage Area
Finding a therapist when mental health professionals are scarce means balancing your need for timely care against the reality of limited availability. The strategies below blend immediate action with longer-term tools, so you can navigate the wait without sacrificing quality.
Start with Telehealth Directories
Begin by expanding your search online. Many directories let you filter specifically for teletherapy, which can unlock clinicians across your state who otherwise work in-person in another city. On Psychology Today, for instance, the "Online Therapy" filter immediately surfaces providers licensed in your state who offer telehealth therapy. Similarly, platforms like GoodTherapy and Zocdoc let you narrow results by insurance, specialty, and telehealth. After you compile a shortlist, call each provider to confirm they accept your plan and are actively taking new patients, even if their online profile says otherwise. Asking to be placed on a waitlist can also pay off, as cancellations often free up slots sooner than expected.
Explore Community-Based Options
If private-practice listings remain thin, turn toward lower-cost, high-volume settings. Community health centers nearly always staff licensed counselors and social workers who treat patients regardless of insurance status, using a sliding-scale fee based on income. University training clinics offer another parallel track: under close supervision, graduate students in psychology or counseling programs deliver care at steeply reduced rates, often $10 to $30 a session. While you may see a clinician in training, the supervision model means your case is discussed with an experienced supervisor, adding a layer of quality control. Search for "community mental health center" or "training clinic" plus your county name to find these resources.
Leverage Interstate Telehealth Compacts
Recent changes in licensure law enable many therapists to practice across state lines via telehealth. The Psychology Interjurisdictional Compact (PSYPACT) allows licensed psychologists to offer telepsychology in member states without obtaining additional licenses, and a similar Counseling Compact is rolling out for mental health counselors. If you live in a participating state, you can legally see a therapist licensed in a neighboring state that has more availability. Check the PSYPACT or Counseling Compact website to confirm your state's status, then use teletherapy directories and select the surrounding states that participate.
Managing the Wait: Interim Support
The gap between starting your search and sitting in a first session can stretch for weeks. During that time, clarify your immediate safety: if you are in crisis, use 988 to reach the Suicide & Crisis Lifeline, or text HOME to 741741. Neither replaces ongoing therapy, but both provide trained listeners in moments of acute distress. For ongoing coping, structured self-help tools such as the CBT-based app Woebot or guided journals can help you track moods and challenge negative thoughts until professional support begins.
Ask About Pre-Licensed Clinicians
A growing number of states are removing insurance billing barriers for pre-licensed therapists, mirroring Hawaii’s Act 93. These associate-level professionals have completed their master’s or doctoral degrees and are accumulating supervised hours for full licensure. Because they can now bill many insurance plans directly, their availability is rising. When you call a practice or clinic, explicitly ask, "Do you have any pre-licensed clinicians who are accepting new patients and are in-network for my insurance?" Their schedules are often more open than those of fully licensed staff, and their work is closely overseen by experienced supervisors.
Frequently Asked Questions About the Mental Health Provider Shortage
With roughly 137 million people in the U.S. living in designated Mental Health Professional Shortage Areas, accessing timely mental health care has become a pressing concern. Here are answers to common questions about navigating the provider shortage.
Future Outlook: What’s Next for the Mental Health Workforce?
Traditional recruitment pipelines alone cannot keep pace with demand. A growing number of states and healthcare systems are turning to innovative care models and technology to bridge the gap.
The Growing Demand-Supply Mismatch
Federal projections paint a stark picture. According to the Health Resources and Services Administration's HRSA workforce projections, demand for behavioral health workers will surge 49% through 2033, while supply grows just 11%. By 2037, the nation could face a deficit of 88,000 to 100,000 mental health counselors and up to 123,000 addiction counselors. The adequacy of addiction counselor supply is expected to be just 21% of what communities need. Within psychiatry, the shortfall is severe: 86,000 adult psychiatrists by 2038, meeting only 30% of projected demand, while child and adolescent psychiatrists will be short by 20,000 (36% adequacy). Psychologists face a 150,000-provider gap. These numbers translate into millions of Americans: 122 million already live in designated shortage areas, waiting months for care or forgoing it entirely.1
Pipeline Pressures and Burnout
The pipeline into the profession remains too narrow. Graduate programs in psychology, social work, and counseling report more qualified applicants than available training slots, particularly for practicum sites. A rapidly aging workforce compounds the problem: roughly 40% of licensed psychologists are over 55 and nearing retirement. Meanwhile, burnout among early- and mid-career professionals is driving attrition. High student debt, low reimbursement rates, and administrative burden push clinicians away from community mental health settings. The supervised experience required for full licensure often becomes a financial dead end, as pre-licensed therapists frequently pay thousands for supervision while earning little or no income.
Shortages in Critical Subspecialties
Not all gaps are felt equally. Specialized fields, including the most needed psychology specialists, face the deepest shortages:
- Child and adolescent: With only 36% adequacy, waitlists for youth therapy and psychiatric evaluation stretch beyond six months in many regions.
- Geriatric mental health: As the population ages, dementia care, late-life depression, and isolation support are critically understaffed.
- School-based providers: The school psychologist shortage already stands at one per 1,500 students in some districts, far above the recommended ratio.
- Addiction treatment: The 21% adequacy rate for substance abuse counselors is especially alarming as the opioid and fentanyl crises continue.
These subspecialty gaps, especially those among the most in-demand counseling specialties, require targeted training investments and loan repayment incentives directed toward high-need settings.
Emerging Solutions on the Horizon
Innovations are reshaping the workforce conversation. AI-assisted therapy tools, including chatbots for structured cognitive behavioral therapy (CBT), are being piloted to extend care for mild-to-moderate conditions and reduce the load on human therapists. Peer support specialist credentialing is gaining traction in Medicaid programs, creating a new tier of frontline support workers with lived experience. Integrated primary care models embed behavioral health consultants in medical settings, allowing warm handoffs and collaborative care. Community health worker programs, often rooted in underserved neighborhoods, bridge cultural and language gaps. Each of these solutions expands team-based care rather than replacing licensed clinicians.
Policy Momentum and the Road Ahead
Bipartisan momentum around workforce legislation is cautiously encouraging. Hawaii's Act 93, signed in 2024 and fully operational by 2026, grants associate-level licenses allowing pre-licensed therapists to bill insurance while earning clinical hours, a direct attack on the supervision cost barrier that pushed graduates out of state.2 Similar bills are advancing in other shortage-heavy states. Combined with telehealth permanence and Medicare reimbursement reforms for mental health counselors, these policy shifts are beginning to move the needle. Sustained progress, however, requires coordinated advocacy from professional organizations, graduate programs, and payers to fund training slots, increase reimbursement, and support the next generation of healers.