
What you’ll learn in this article…
- Over 160 million Americans live in federally designated Mental Health Professional Shortage Areas as of 2026.
- Licensure takes 2.5 to 4 years after a master's degree, creating a slow pipeline that widens the gap.
- Substance abuse and child or adolescent counseling specialties face the steepest projected shortfalls through 2038.
- Telehealth credentials, Counseling Compact licensure, and NHSC loan repayment sites give new graduates a strategic edge.
More than 165 million Americans live in federally designated Mental Health Professional Shortage Areas, according to the Health Resources and Services Administration. That figure is not a projection; it reflects current, documented gaps in provider supply across rural counties, underserved urban neighborhoods, and correctional facilities alike.
For counseling students, this reality cuts two ways. The shortage is a genuine public health crisis, one driving longer wait times, undertreated conditions, and overburdened providers. It is also the defining career condition for a new generation of clinicians: demand is structurally high, and HRSA projects that gap will widen through the late 2030s under current training and retention trends.
The practical tension is not whether jobs exist. It is how to enter this workforce strategically, choosing the right specialty, state, and credential pathway to avoid the traps that keep many new counselors underpaid and overextended despite high demand. Understanding the landscape of best masters in mental health counseling programs is one of the first steps toward making that strategy work.
How Severe Is the Mental Health Workforce Shortage?
How many Americans actually live in areas without enough mental health providers, and how large is the projected gap between supply and demand?
The answer is sobering. The shortage of mental health professionals in the United States is not speculative or anecdotal. It is measured, federally designated, and projected to worsen over the next decade.
More Than 137 Million Americans Live in Shortage Areas
The Health Resources and Services Administration (HRSA) designates Health Professional Shortage Areas (HPSAs) for communities that lack adequate provider coverage. As of late 2025, roughly 137 million people, about 40% of the U.S. population, live in areas designated as mental health HPSAs.1 To put that in perspective, the comparable figure for primary care HPSAs is approximately 92 million, and for dental HPSAs it is around 64 million.2 Behavioral health shortages affect a larger share of the population than either of those better-known gaps.
These designations are not abstract labels. They translate directly into longer wait times, higher caseloads for existing providers, and entire counties where a licensed therapist or counselor simply does not practice.
Federal Projections Through 2038
HRSA's 2025 behavioral health workforce projections estimate national shortfalls across every major counseling discipline by 2038:1
- Mental health counselors: projected shortfall of approximately 99,780
- Psychologists: projected shortfall of approximately 99,840
- Addiction counselors: projected shortfall of approximately 77,050
- Marriage and family therapists: projected shortfall of approximately 33,840
- Mental health and substance use disorder social workers: projected shortfall of approximately 17,030
Combined, these projections point to a gap of more than 327,000 behavioral health professionals within roughly a dozen years. The scale of this deficit is difficult to overstate.
Demand Is Accelerating, Not Leveling Off
The Bureau of Labor Statistics projects that employment for substance abuse, behavioral disorder, and mental health counselors will grow significantly faster than the average for all occupations over the 2024 to 2034 period. That growth rate reflects both structural demand (aging populations, expanded insurance parity laws) and the sustained post-pandemic surge in utilization. Students weighing a mental health counselor career should know that this trajectory shows no signs of slowing.
Since 2020, therapy utilization has climbed sharply. Insurance claims for mental health services rose substantially across commercial and public payers, and provider waitlists in many regions stretched from weeks to months. While some of the initial pandemic-era spike has stabilized, utilization rates have not returned to pre-2020 baselines. The cultural shift toward seeking mental health care appears durable.
The Direct Answer
Is there a therapist shortage? Yes. It is documented by federal workforce data, projected to persist through at least 2038, and affects communities in every region of the country. For students considering a career in counseling, this context matters: you are entering a field where trained professionals are urgently needed, and the gap between supply and demand continues to widen. Understanding where and how this shortage manifests can help you make strategic decisions about specialization, geography, and the credentials that will serve you and your future clients best.
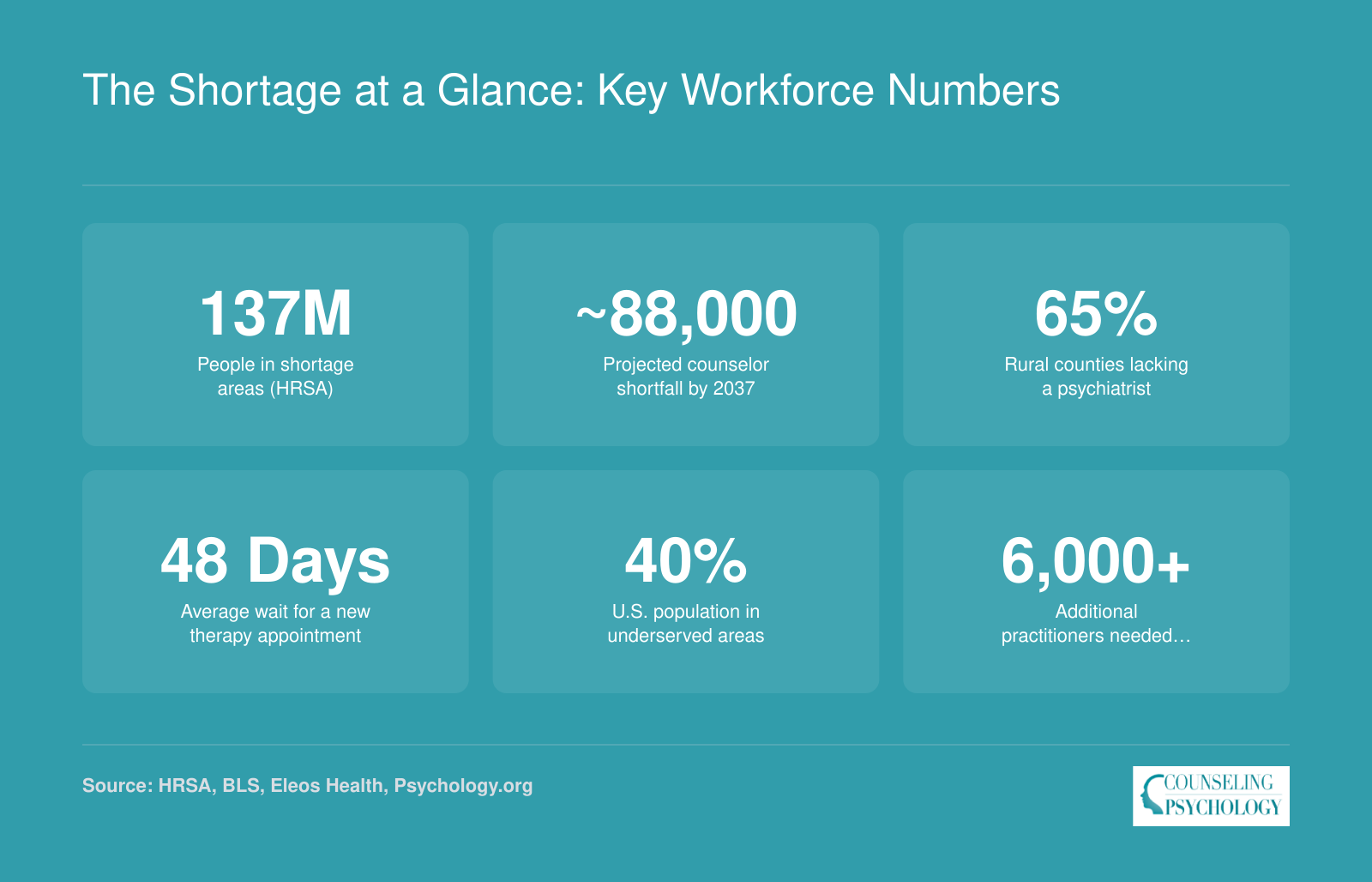
The Shortage at a Glance: Key Workforce Numbers
The scale of the mental health workforce gap touches every corner of the country. These headline figures illustrate how deep the shortfall runs and why demand for new counselors continues to accelerate.
Why the Therapist Shortage Keeps Growing
Becoming a fully licensed mental health counselor takes an average of 2.5 to 4 years after completing a master's degree, and that gap alone explains much of the pipeline problem.1 The shortage is not simply a matter of too few people entering the field. It reflects a series of structural obstacles that slow workforce entry, push out experienced clinicians, and thin the ranks of senior practitioners who train the next generation.
The Training Bottleneck
Before a graduate student logs a single supervised hour toward licensure, they need a practicum or internship placement. In many regions, those sites are scarce. Community mental health centers, school systems, and hospital departments have limited bandwidth to host and supervise trainees, and full licensure typically requires 2,000 to 4,000 supervised post-degree hours depending on the state. Finding qualified supervisors willing to take on that load is a persistent problem in rural and underserved areas. The result: graduates who are ready and motivated wait months, sometimes longer, before they can accumulate hours, and the licensed workforce grows more slowly than demand requires.
State licensing requirements add another layer of friction. Requirements for supervised hours, acceptable supervision formats, and approved coursework vary considerably from one state to the next. A counselor who trains in one state and moves to another can face additional hurdles that delay independent practice. Students interested in understanding the full licensed professional counselor pathway should factor these interstate differences into their planning. That inconsistency discourages geographic mobility and concentrates new clinicians in markets that already have the most training infrastructure.
Burnout Is Draining the Existing Workforce
Among behavioral health workers nationally, a 2023 survey found that 93 percent reported burnout symptoms, and nearly half (48 percent) indicated an intention to leave their current role.2 Among therapists specifically, burnout has been linked to a 27 percent increase in turnover rates.3 Clinicians in community mental health counselor roles face particularly heavy administrative loads, with documentation and compliance tasks consuming roughly 35 percent of their working hours.2 That time comes directly out of patient care capacity and professional satisfaction.
Child therapists report the highest burnout rates among clinical subgroups at 61 percent, followed by school counselors at 55 percent.3 High caseloads, limited organizational support, and inadequate compensation in publicly funded settings push experienced counselors toward private practice or out of direct service entirely, narrowing access for the communities that need care most.
A Retirement Wave at the Top
At the same time experienced mid-career clinicians are burning out, the profession is also losing its most senior practitioners. Baby-boomer-era psychologists and psychiatrists are retiring in significant numbers, removing not just clinical capacity but also the supervisors and mentors who support new counselors through the licensure process. When a senior clinician retires, the loss ripples through the training pipeline as well as the direct service roster.
Demand Is Rising While Supply Lags
Post-pandemic mental health awareness has driven more people to seek care. Mental health parity laws have expanded insurance coverage. Telehealth expansion has theoretically broadened reach. Yet supply-side constraints mean that roughly 40 percent of the U.S. population lived in a designated mental health shortage area as of 2025, with an average of 320 individuals for every one mental health provider. Projections from HRSA suggest the shortfall in mental health counselors could reach 88,000 by the late 2030s, with addiction counselors facing an even steeper gap of approximately 114,000.5 Without structural changes to training capacity, licensure pathways, and retention, rising demand will continue to outpace the profession's ability to produce new clinicians.
Questions to Ask Yourself
Counselor Shortage by Specialty: Where Demand Is Highest
Not every counseling specialty faces the same workforce gap. HRSA projections through 2038 show that some fields will meet less than a third of projected demand under current training and retention trends, while others hover closer to adequacy. The table below pairs those shortage estimates with BLS employment and salary data so you can see where the need, and the opportunity, is greatest.
| Specialty | Projected Shortfall by 2038 | Workforce Adequacy (2038) | Current National Employment | National Median Salary (BLS) |
|---|---|---|---|---|
| Psychologists (Clinical and Other) | -99,840 | 48% | N/A | N/A |
| Mental Health Counselors | -99,780 | 55% | 440,380 (combined with substance abuse and behavioral disorder counselors) | $59,190 (combined category) |
| Addiction / Substance Abuse Counselors | -77,050 | 30% | Included in combined BLS category above | Included above |
| School Counselors | -39,680 | 80% | 342,350 (educational, guidance, and career counselors and advisors) | $65,140 |
| Marriage and Family Therapists | -33,840 | 60% | N/A | N/A |
How the Shortage Affects Students and Communities
Only 25 percent of school counselors nationally carry a caseload at or below the American School Counselor Association's recommended 250-to-1 ratio, according to ASCA survey data.1 That means three out of four counselors are stretched beyond what the profession's own evidence base considers safe.
What the Numbers Look Like in Schools
For the 2024-25 school year, the national average student-to-counselor ratio sits at 372 to 1, nearly 50 percent above the recommended ceiling.1 The gaps widen dramatically at certain grade levels. At the elementary and middle school level, ratios range from 571 to 1 up to 694 to 1 nationally, which means hundreds of younger students share a single counselor.1 Arizona's statewide ratio reaches 570 to 1, one of the highest in the country.2 Vermont, by contrast, comes in at 172 to 1, below the recommended threshold.2 Colorado (247 to 1) and Hawaii (243 to 1) are among the states close to compliance, while most of the country falls well short.1
How Ratios Translate into Real Outcomes
Research consistently links elevated ratios to measurable harm. Students in under-resourced schools show lower rates of college enrollment and reduced access to early identification when warning signs of crisis or academic failure appear. When one counselor is responsible for 500 or 600 students, there is simply no capacity for proactive outreach. Crisis response slows. Students who might have been redirected earlier arrive at more acute stages of distress.
Community-Level Consequences
Beyond K-12 settings, the shortage reshapes how communities access mental health care overall. Adults seeking therapy in many areas wait weeks, not days, before a first appointment becomes available. That delay pushes some people toward emergency departments for psychiatric crises, a more expensive and often less effective point of intervention. Rural communities feel this most acutely: provider density is lower, transportation barriers are real, and teletherapy coverage remains inconsistent.
An Equity Gap That Compounds the Problem
Communities of color and low-income neighborhoods face layered disadvantages. Fewer providers hold bilingual or bicultural competencies, which limits genuine therapeutic access even where a provider technically exists. Research on the availability of BIPOC therapists confirms that representation gaps persist across much of the profession. Rural areas combine geographic isolation with lower reimbursement rates, which discourages providers from setting up practice there. The shortage is not evenly distributed; it concentrates precisely in the places where need tends to be highest and existing resources are already thin.
Related Articles
Where Counseling Jobs Are Most Needed: A Regional Salary and Employment Outlook
The table below focuses on substance abuse, behavioral disorder, and mental health counselors (BLS occupation 21-1018), the category most directly relevant to students entering clinical mental health or substance abuse counseling. States with the largest workforces are not necessarily the highest paying, and many of the highest-employment states still contain vast federally designated Health Professional Shortage Areas, particularly across rural counties. When evaluating pay, keep in mind that top-median states like Alaska, New Mexico, and Oregon carry elevated costs of living that absorb part of the salary premium, while states like North Dakota and Idaho may offer stronger purchasing power despite lower nominal wages.
| State | Total Employment | Median Annual Salary | 25th Percentile Salary | 75th Percentile Salary |
|---|---|---|---|---|
| New York | 22,450 | $62,070 | $50,880 | $76,680 |
| New Jersey | 14,640 | $64,710 | $51,170 | $84,690 |
| Washington | 13,150 | $64,220 | $52,070 | $80,440 |
| Wisconsin | 9,450 | $62,470 | $50,870 | $77,800 |
| Arizona | 8,970 | $63,830 | $50,650 | $79,990 |
| Connecticut | 6,470 | $62,960 | $49,120 | $77,610 |
| Oregon | 6,410 | $69,660 | $56,290 | $84,970 |
| Utah | 4,720 | $65,920 | $42,210 | $94,630 |
| Idaho | 2,130 | $65,240 | $48,570 | $78,100 |
| New Mexico | 2,070 | $70,770 | $55,060 | $80,840 |
| Nebraska | 1,980 | $64,410 | $46,900 | $81,210 |
| North Dakota | 1,180 | $66,450 | $50,810 | $75,120 |
| Alaska | 1,060 | $79,220 | $63,690 | $96,940 |
| District of Columbia | 980 | $66,140 | $47,980 | $83,040 |
| Wyoming | 840 | $61,640 | $42,610 | $79,830 |
Salary, Caseloads, and Working Conditions in High-Demand Areas
The national median wage for substance abuse, behavioral disorder, and mental health counselors sits at approximately $53,000, according to Bureau of Labor Statistics data. That baseline figure, however, masks significant geographic variation and tells only part of the story for counseling students entering the workforce during a national shortage. Understanding the compensation-versus-caseload tradeoff is essential career-planning intelligence: higher pay does not always mean better working conditions, and high-need areas often come with heavy workloads that can accelerate burnout.
Geographic Pay Variation and the Cost-of-Living Calculus
Metropolitan areas at the top of the wage distribution can exceed the national median by fifteen to twenty thousand dollars. Mental health counselors in San Francisco-Oakland earn a median of approximately $72,950, while those in New York-Newark-Jersey City report a median near $64,900. Boston-Cambridge-Newton and Washington-Arlington-Alexandria also cluster in the mid-to-high sixties. Yet each of these metros ranks among the nation's most expensive housing markets. A twenty-thousand-dollar salary premium in San Francisco buys significantly less purchasing power than the national median in a mid-sized city with moderate rent. Students evaluating job offers should calculate take-home pay after housing, not just compare advertised salaries. For a deeper breakdown of pay by degree level and specialty, see our guide to counselor salary with masters. Mental health and substance abuse social workers in New York command a median of $83,490, but rent for a one-bedroom apartment in the metro can consume forty percent or more of gross income.
Caseload Realities in Community Mental Health
Community mental health centers and nonprofit agencies in high-demand areas routinely assign caseloads of thirty to forty active clients per counselor, and some clinics push that figure higher during staffing shortages. These numbers contrast sharply with private-practice norms, where ten to twenty clients per week is common, or school counseling, where ratios can range from one counselor per two hundred fifty students to one per five hundred, depending on state funding. Research on counselor burnout consistently links caseload size to emotional exhaustion and turnover. A federally qualified health center in a rural shortage area may offer loan repayment through the National Health Service Corps and a signing bonus of five to ten thousand dollars, yet the position may also require seeing eight to ten clients per day with minimal administrative support. Students should ask practicum sites and potential employers not only about starting salary but also about typical caseload, supervision structure, administrative time, and staff retention rates.
The Loan Repayment and Incentive Trade
National Health Service Corps loan repayment can cover up to fifty thousand dollars over two years for clinicians working in designated Health Professional Shortage Areas. State-level programs in California, Texas, New York, and other high-need states add additional incentives. These benefits substantially improve the financial calculus for graduates carrying sixty thousand dollars or more in student debt. However, loan repayment is not a substitute for sustainable working conditions. A counselor who burns out after eighteen months loses both the remainder of the repayment benefit and the professional momentum needed to build a long-term career. Weighing these tradeoffs requires honest self-assessment during the job search: can you sustain a forty-client caseload for two years in exchange for debt relief, or will a lower-volume private practice with slower debt payoff preserve your capacity to stay in the field?
High demand does not automatically translate to high pay. The smartest move is pairing a high-need specialty with strategic positioning: telehealth credentials, licensure in Counseling Compact states, and placement at NHSC loan repayment sites. That combination turns the shortage into both genuine job security and sustainable working conditions over the long haul.
How to Position Yourself as a Counseling Student
Strategic decisions made during your counseling program can determine whether you land a job in six weeks or six months, whether you qualify for loan repayment, and whether you can practice across state lines via telehealth. The workforce shortage creates opportunity, but only if you build the credentials, specializations, and competencies that employers and insurers demand.
Choose a CACREP-Accredited Program
CACREP accreditation is no longer optional for most counseling careers. Thirty-four states now require or prefer CACREP-accredited master's degrees for licensure as a professional counselor, and that number continues to grow. More importantly, the Counseling Compact (which we'll discuss below) requires a CACREP-accredited degree to participate. Employers and managed-care panels increasingly list CACREP as a minimum qualification. Non-CACREP programs may be cheaper or more convenient, but they close doors. If you're already enrolled in a non-CACREP program, check whether your school is in candidacy status or plans to seek accreditation before you graduate. Students exploring accredited options can compare online clinical mental health counseling programs to find the right fit.
Target High-Demand Specializations
The shortage is not uniform. Demand is most acute in addiction counseling, child and adolescent therapy, trauma-informed care, and school counseling. If your program offers a concentration or elective track in one of these areas, take it. Practicum and internship placements in these specialties signal readiness to hiring managers. Those drawn to working with younger populations should explore what it takes to become a child counselor, since school counseling deserves special mention: the national shortage of school counselors exceeds 14,000 positions, and many states are now approving provisional licenses or alternative pathways to fill the gap. Graduates with a school counseling credential often receive multiple job offers before graduation.
Understand the Counseling Compact and Plan for Portability
The Counseling Compact allows licensed professional counselors to practice across state lines without obtaining multiple licenses.1 As of April 2026, 39 states and the District of Columbia have enacted compact legislation.2 Four states (Arizona, Louisiana, Minnesota, and Ohio) are fully operational, and 35 additional states are in various stages of implementation.3 Once a counselor holds an independent license in their home state (a compact member), they can apply through the Compact Commission's online system for a privilege to practice in any other live compact state. That privilege enables telehealth sessions with clients located in the remote state, governed by that state's scope-of-practice rules.3 Provisional and supervised licenses do not qualify; you must complete all postgraduate supervision and hold full independent licensure. If you plan to offer telehealth or relocate, prioritize programs in compact member states and choose practicum sites that incorporate virtual sessions.
Build Telehealth Competency During Training
Telehealth is now standard practice, not a pandemic workaround. Practicum and internship sites that offer virtual sessions give you hands-on experience with videoconferencing platforms, remote assessment, and the unique dynamics of online counseling. Graduates who list telehealth experience on their résumés stand out. If your program does not offer virtual practicum placements, ask your clinical coordinator to add them.
Consider NHSC-Eligible Practicum Sites and Underserved Areas
Practicum and internship placements in Health Professional Shortage Areas or NHSC-approved sites serve two purposes: they meet your clinical hours requirement and position you for federal loan repayment. The National Health Service Corps offers up to $75,000 in loan repayment for counselors who commit to two or three years in underserved communities. Many graduates who complete practicum in these settings are offered full-time positions immediately after licensure, because the site already knows their clinical work and has an urgent need. Check the NHSC site locator and ask your program coordinator which practicum placements qualify.
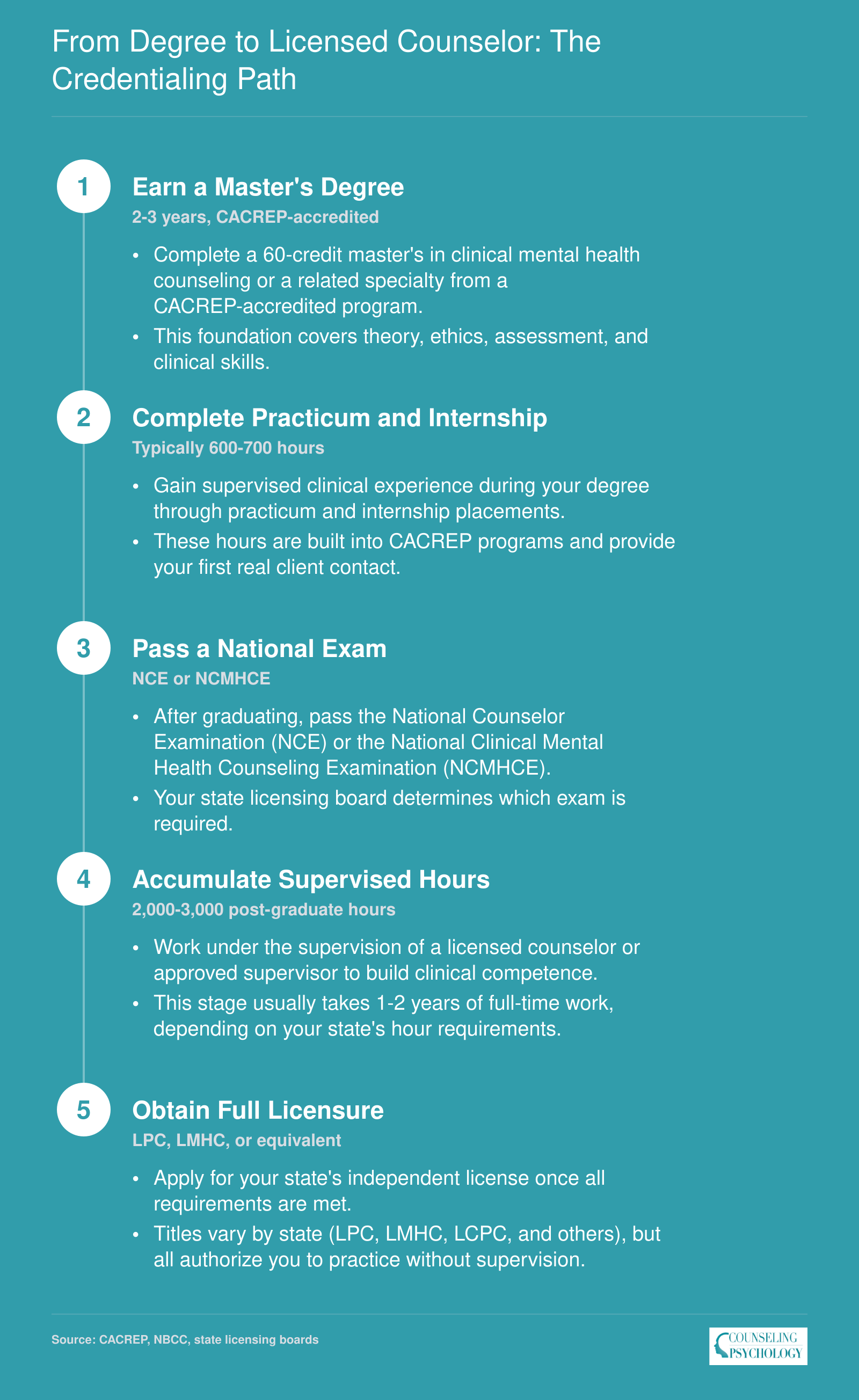
From Degree to Licensed Counselor: The Credentialing Path
The path from graduate student to independently licensed counselor follows a predictable sequence, but each stage takes real time and effort. Most aspiring counselors should plan on 4-6 years from the start of their master's program to full independent licensure.
Frequently Asked Questions About the Mental Health Workforce Shortage
The mental health workforce shortage raises practical questions for anyone considering a counseling career. Below are answers to the most common ones, grounded in current workforce data and policy developments.