What you’ll learn in this article…
- Only about 4 percent of U.S. psychologists are Black, while Black Americans represent roughly 13 percent of the population.
- Clients matched with a racially concordant therapist are four times more likely to remain in treatment.
- Clinical social work leads all mental health disciplines in BIPOC representation at approximately 30 percent.
- Riverside, CA illustrates the shortage: roughly one MFT serves every 2,000 residents in a majority BIPOC metro.
BIPOC Americans make up roughly 40% of the U.S. population, yet only about 20% of the mental health workforce identifies as BIPOC. That gap is not a coincidence. It reflects compounding barriers: graduate school costs, licensure timelines that stretch three to five years beyond a master's degree, and a field that has historically centered the experiences of white, middle-class clients.
The mismatch has measurable consequences. Research consistently links racial and ethnic concordance between therapist and client to better treatment retention, stronger therapeutic alliance, and more accurate diagnosis. For communities already navigating distrust of medical institutions, the shortage of culturally affirming providers is not a minor inconvenience. It shapes whether people seek help at all.
The workforce is growing, but supply has not kept pace with demographic reality or documented need.
How Many Black Therapists Are There in the U.S.?
Where do you actually find reliable counts of Black therapists working in the United States today?
The short answer: no single registry tracks all practicing therapists by race. Mental health professionals are licensed across four major disciplines (psychologists, licensed professional counselors, clinical social workers, and marriage and family therapists), each with its own credentialing body and data collection practices. To piece together the national picture, you need to consult multiple sources and understand what each one measures.
Psychologists: APA and BLS Data
The American Psychological Association's Center for Workforce Studies conducts periodic demographic surveys of licensed psychologists and doctoral students. As of the most recent publicly available survey cycle, approximately 5 percent of practicing psychologists in the United States identify as Black or African American. The Bureau of Labor Statistics groups clinical, counseling, and school psychologists into a single occupational category but does not routinely publish race-specific breakdowns in its standard employment reports. For more granular workforce data, the APA survey remains the authoritative source. Those interested in the broader profession can explore careers in psychology for additional context on the field's scope and specializations.
Licensed Professional Counselors: AMHCA and NBCC
The American Mental Health Counselors Association and the National Board for Certified Counselors collect membership and certification demographics. NBCC's most recent diversity report indicates that roughly 6 to 7 percent of nationally certified counselors identify as Black. Because professional counselor licensure is state-administered, some state boards publish demographic summaries of their licensee pools. These state-level reports can reveal meaningful regional variation but are not aggregated at the national level in a single, publicly accessible database.
Clinical Social Workers: NASW and State Boards
The National Association of Social Workers maintains membership demographics showing that approximately 9 percent of NASW members identify as Black or African American. However, NASW membership is voluntary and does not capture all licensed clinical social workers. For a more complete count, you would need to cross-reference state licensure databases, many of which do not publish race or ethnicity data publicly due to privacy and administrative limitations.
Marriage and Family Therapists: AAMFT Workforce Survey
The American Association for Marriage and Family Therapy periodically surveys its membership and finds that approximately 4 to 5 percent of respondents identify as Black. Like other professional associations, AAMFT's data reflects its membership base rather than the full universe of state-licensed MFTs. If you are considering this path, our guide on how to become a marriage and family therapist outlines the steps involved.
U.S. Census Bureau and Community Surveys
The American Community Survey publishes occupation-by-race tables that include broad categories such as "Counselors" and "Social Workers." These self-reported figures do not distinguish clinical specialties or licensure status, so they are most useful for understanding the overall occupational landscape rather than for counting licensed practitioners. Nonprofits such as the Black Mental Health Alliance and university research centers occasionally publish localized or aggregated counts, but these remain snapshots rather than comprehensive registries.
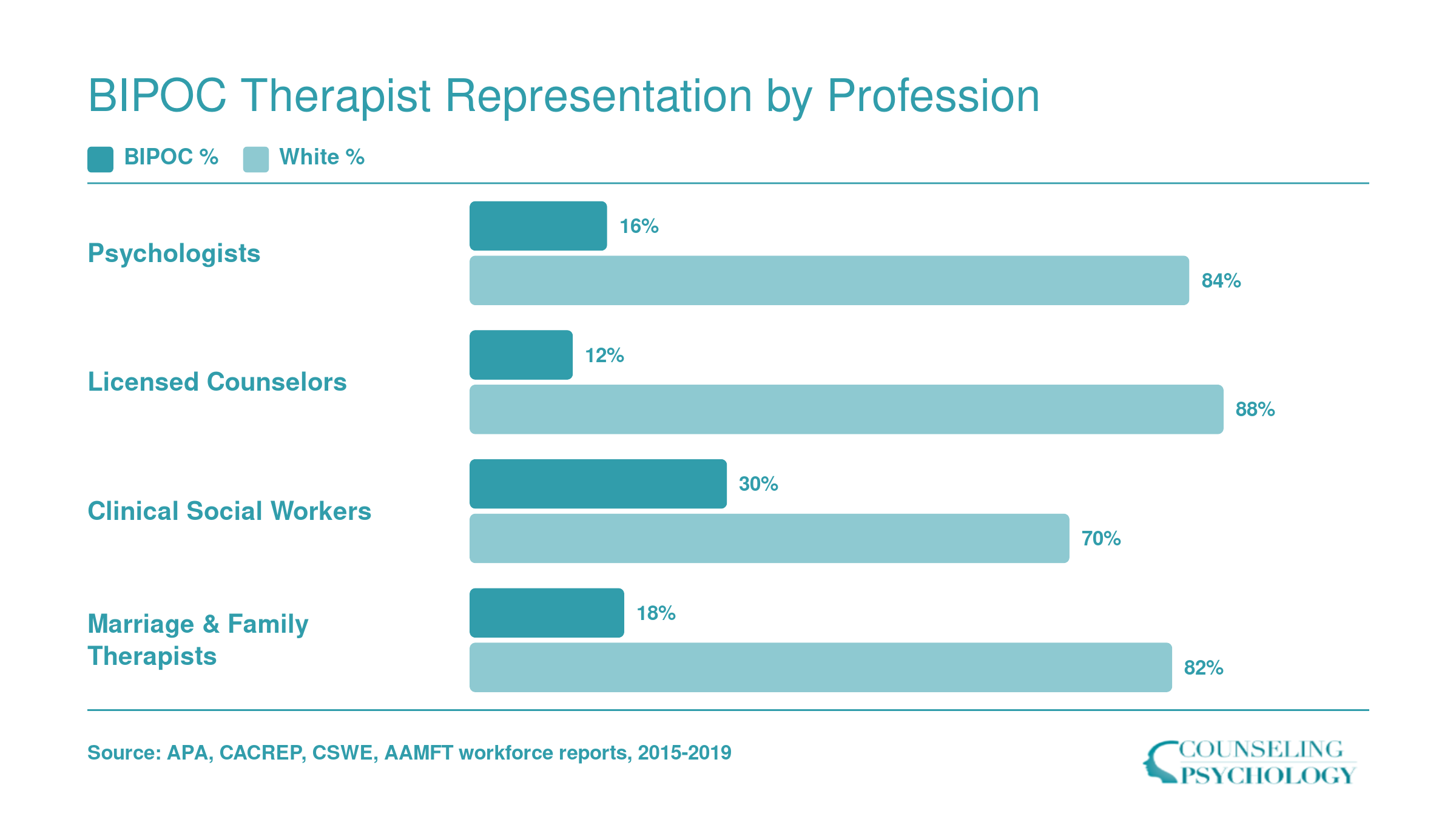
Across all four disciplines, the data converge on a consistent finding: Black therapists represent between 4 and 9 percent of their respective professions, even though Black Americans constitute roughly 13 percent of the U.S. population.
BIPOC Therapist Representation by Profession
The gap between BIPOC and White representation varies sharply depending on which mental health profession you examine. Clinical social work leads all four disciplines in BIPOC representation at roughly 30%, partly because social work training has historically centered community-based practice in underserved neighborhoods. That broader pipeline matters: higher BIPOC representation in social work means more culturally concordant providers are available in the communities that need them most.
Why Are There so Few Black and BIPOC Therapists?
Twenty-five percent of students in APA-accredited counseling programs identified as students of color in 1995, a proportion that has grown in subsequent decades but still fails to match the demographic composition of communities most in need of mental health services.1 The shortage of Black and BIPOC therapists stems from a multi-stage pipeline problem that begins long before licensure and persists throughout clinical careers.
Financial Barriers Block Entry to Graduate Programs
The cost of graduate training in clinical psychology, counseling, and social work creates the first obstacle. Doctoral candidates in clinical psychology frequently graduate with six-figure student debt, while master's-level counseling and social work students face tuition bills ranging from thirty to seventy thousand dollars for a two- or three-year program. Students exploring counseling master's programs online will find wide variation in cost, but BIPOC students are more likely to carry undergraduate debt into graduate school, compounding the financial burden and deterring otherwise qualified candidates from entering the field. Many BIPOC students cannot afford to forgo income during unpaid or low-wage practicum placements, a standard requirement in counseling and social work training.
Lack of Mentorship and Hostile Training Climates
Faculty representation matters. BIPOC students in counseling programs report difficulty finding mentors who share their lived experience or understand the cultural contexts that shape their clinical interests. When faculty and supervisors are overwhelmingly white, students of color often find themselves educating peers and instructors about race rather than receiving guidance. Training environments that fail to address microaggressions, tokenize BIPOC students, or treat multicultural counseling as an optional elective rather than a core competency push students out before degree completion. CACREP Vital Statistics reports indicate that Clinical Mental Health Counseling is the largest specialty area within accredited programs, yet attrition rates for BIPOC students in these tracks remain higher than for white peers.2
Retention Challenges After Licensure
Even when BIPOC therapists complete training and earn licensure, the field struggles to retain them. BIPOC clinicians disproportionately work as community mental health counselors, in school-based programs, and at nonprofit agencies where salaries lag far behind private practice rates. Burnout compounds the pay gap: BIPOC therapists frequently carry a disproportionate caseload of clients experiencing racial trauma, immigration stress, and systemic oppression, yet few have access to clinical supervisors who share their racial or ethnic background and can provide culturally grounded support.
Historical Mistrust and Psychology's Legacy
Psychology's history of pathologizing Black identity and other non-white identities erects a trust barrier that discourages young BIPOC students from entering the profession. For decades, diagnostic manuals and research framed racial and cultural differences as deficits. This legacy persists in training curricula that center Eurocentric theories and ignore the contributions of scholars of color, reinforcing the perception that the field is not built for or by BIPOC clinicians.
Related Articles
Questions to Ask Yourself
Benefits of Seeing a Culturally Concordant Therapist
A 2011 meta-analysis by Cabral and Smith, published in the Journal of Counseling Psychology, examined 81 studies and found that clients paired with racially or ethnically matched therapists were four times more likely to remain in treatment compared to those in non-matched dyads. That retention advantage translates directly into better outcomes, because therapy works only when clients stay engaged long enough for therapeutic techniques to take hold.
Racial and ethnic concordance between therapist and client (a Black therapist working with a Black client, or a Latina counselor with a Latinx client) has been studied extensively over the past three decades, and the evidence consistently points to measurable benefits across multiple dimensions of care.
Stronger Therapeutic Alliance
The therapeutic alliance, the collaborative bond between client and therapist, predicts outcomes more reliably than any single treatment modality. Research published in Cultural Diversity and Ethnic Minority Psychology and Psychotherapy shows that racially concordant dyads often establish trust more quickly. Shared lived experience with discrimination, microaggressions, or cultural norms reduces the explanatory burden on clients. They spend less time educating their therapist about context and more time addressing the presenting problem. A 2018 study in the Journal of Counseling Psychology found that Black clients working with Black therapists reported higher alliance scores within the first three sessions than those in non-matched pairs.
Higher Retention and Treatment Completion
Beyond the Cabral and Smith findings, subsequent analyses have confirmed that clients of color drop out of therapy at lower rates when their therapist shares their racial or ethnic background. University research teams at institutions with strong psychology and social work departments, including those affiliated with the American Psychological Association and the American Counseling Association, have documented this pattern in community mental health centers, private practice settings, and university counseling centers alike. When clients feel understood without constant code-switching or justification, they commit to the work.
Symptom Reduction and Client Satisfaction
Peer-reviewed studies accessible through PsycINFO and PubMed show that culturally concordant therapy correlates with faster symptom improvement in depression and anxiety. Professionals pursuing a career as a depression counselor should be especially aware of this evidence, since therapeutic match can meaningfully influence treatment timelines. Client satisfaction scores, measured via post-session surveys and treatment-exit interviews, run consistently higher in matched dyads. Professional association websites, including those of the American Mental Health Counselors Association, publish practice guidelines and research summaries that synthesize this evidence for clinicians seeking to improve care for BIPOC populations.
Where to Find the Research
Meta-analyses and original studies appear regularly in journals like Cultural Diversity and Ethnic Minority Psychology, the Journal of Counseling Psychology, and Psychotherapy. Google Scholar searches return synthesized evidence from reviews dating back to the early 2000s. University psychology and social work department faculty pages often list publications on cultural competence and client-therapist matching. Students exploring degrees in psychology will find that many programs now integrate this literature into their core curricula, offering a direct line to the latest empirical work in this area.
Cities Where BIPOC Therapists Best Serve Their Communities
Several major metro areas combine high marriage and family therapist (MFT) employment with median salaries that can sustain a viable practice, and many of these same cities are home to large, diverse populations. Metros with robust community mental health infrastructure, including publicly funded clinics, university training sites, and nonprofit counseling centers, tend to cluster in this list. The table below focuses on MFT employment because that occupation aligns most directly with the counseling and therapy workforce discussed throughout this article. Salary figures reflect BLS data for each specific metro area, not national medians.
| Metro Area | Total MFT Employment | Median Annual Salary | 25th Percentile Salary | 75th Percentile Salary |
|---|---|---|---|---|
| Los Angeles, Long Beach, Anaheim, CA | 12,400 | $64,420 | $47,050 | $91,580 |
| San Francisco, Oakland, Fremont, CA | 3,400 | $76,980 | $57,980 | $104,970 |
| New York, Newark, Jersey City, NY/NJ | 2,900 | $86,120 | $70,660 | $97,670 |
| San Diego, Chula Vista, Carlsbad, CA | 4,660 | $48,950 | $48,950 | $75,750 |
| Minneapolis, St. Paul, Bloomington, MN/WI | 2,490 | $72,910 | $59,780 | $83,830 |
| Riverside, San Bernardino, Ontario, CA | 2,200 | $60,780 | $45,260 | $79,030 |
| Philadelphia, Camden, Wilmington, PA/NJ/DE/MD | 2,060 | $80,090 | $62,830 | $89,030 |
| Sacramento, Roseville, Folsom, CA | 1,270 | $72,810 | $49,010 | $96,480 |
| San Jose, Sunnyvale, Santa Clara, CA | 1,220 | $88,950 | $59,560 | $123,430 |
In 2017, Black students earned just 5.8 percent of psychology doctoral degrees nationally, while Latino students earned 7.3 percent. Combined, these two groups represented barely 13 percent of new doctoral psychologists despite comprising over 30 percent of the U.S. population. Growth has occurred, but the pace has not matched the urgent need for culturally concordant care.
Cities Where BIPOC Communities Are Underserved by Therapists
Riverside-San Bernardino-Ontario, CA reports only 2,200 marriage and family therapists for a metro of roughly 4.6 million residents, where Hispanic, Black, and Asian residents together account for more than 60% of the population. That ratio, roughly one MFT per 2,000 residents, lags far behind metros with similar populations but smaller BIPOC shares.
Where the Supply-Demand Gap Is Widest
Using the BLS Occupational Employment and Wage Statistics metro file as a foundation, several large metros stand out for thin therapist supply relative to their BIPOC populations:
- Riverside-San Bernardino-Ontario, CA: 2,200 MFTs serving a metro that is over 50% Hispanic. Per-capita therapist employment is well below the California state average.
- Houston-Pasadena-The Woodlands, TX: The metro does not even register in the top BLS reporting tiers for marriage and family therapists, despite a population of 7.3 million that is roughly 45% Hispanic and 17% Black.
- Dallas-Fort Worth-Arlington, TX: Similar pattern. Occupational therapist and physical therapist counts are robust (3,160 and 4,570 respectively), but the mental health therapist workforce is comparatively sparse for a metro that is nearly half BIPOC.
- Miami-Fort Lauderdale-West Palm Beach, FL: Heavy Hispanic and Caribbean Black populations, yet the metro likewise falls short of California or Northeast metros in MFT employment density.
- San Bernardino and Inland Empire counties: A documented mental health professional shortage area per HRSA designations.
What the Shortage Looks Like on the Ground
When a metro has 40% or more BIPOC residents but a therapist-to-resident ratio at half the national average, the consequences are concrete. Wait times for an intake appointment can stretch six to twelve weeks at community clinics. Patients in acute distress end up routed to emergency departments, which were never designed for sustained mental health care. Those interested in addressing these gaps should understand the full scope of community mental health counselor roles, which are among the most in-demand positions in underserved areas. Crisis hotlines and mobile crisis teams pick up overflow that outpatient therapists should be handling. For BIPOC residents specifically, the shortage of culturally concordant providers compounds the wait: even when an appointment exists, it may not be with someone who shares the client's language or lived experience.
Telehealth as a Partial Bridge
Since 2020, telehealth has expanded the geographic reach of therapists licensed in a given state. A Black therapist based in Sacramento can now see clients across California, including underserved Inland Empire ZIP codes. Interstate compacts like PSYPACT for psychologists and the Counseling Compact for LPCs are slowly extending that reach across state lines. Telehealth does not solve the underlying workforce shortage, but it does redistribute existing supply toward the metros that need it most. For professionals weighing their options, exploring careers in mental health counseling can clarify where the greatest demand exists.
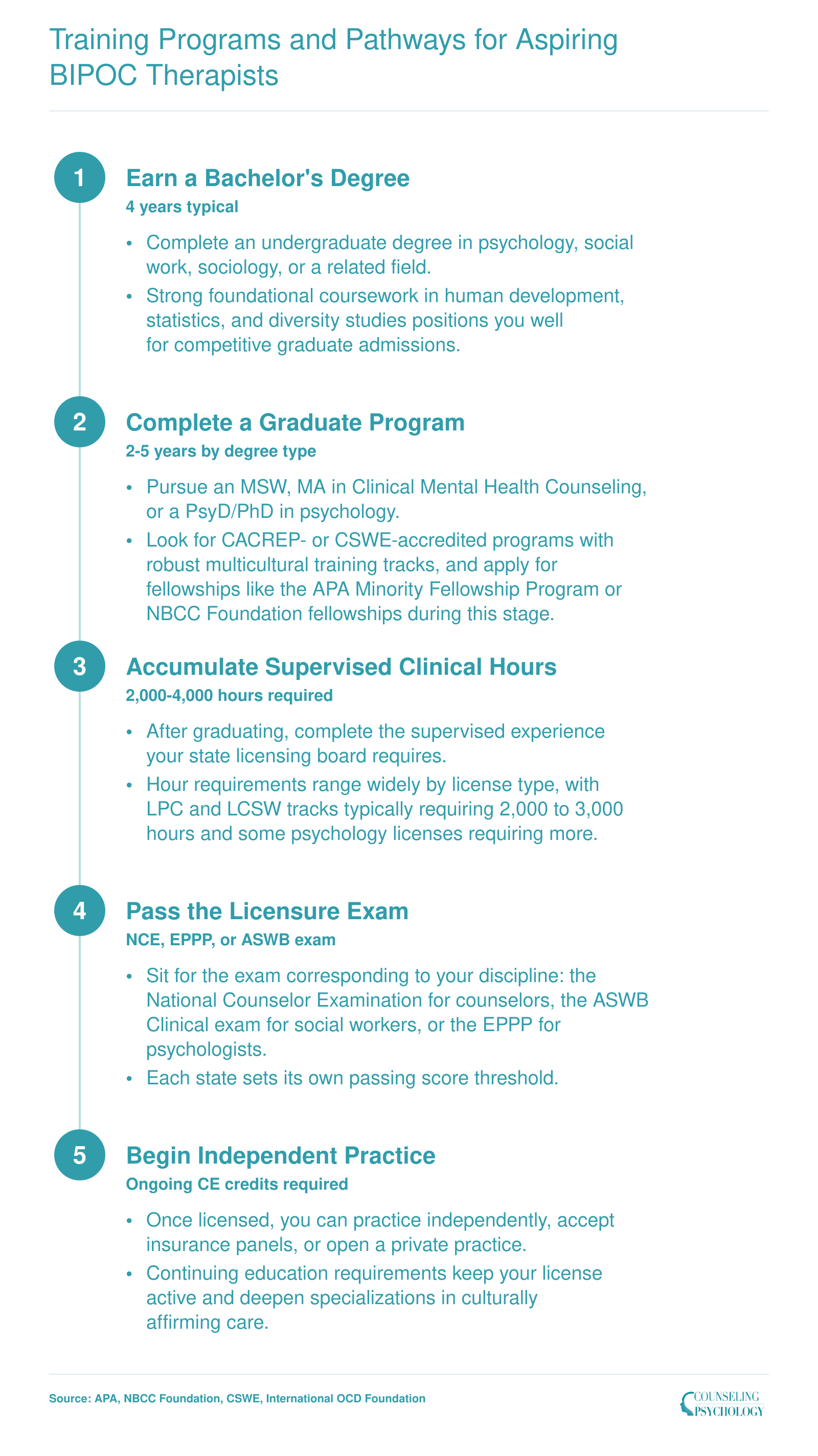
Training Programs and Pathways for Aspiring BIPOC Therapists
The road from undergraduate coursework to independent clinical practice follows a well-defined sequence, though the timeline shifts depending on whether you pursue an MSW, an MA in counseling, or a doctoral degree. Several fellowships and scholarships exist specifically to support BIPOC students along this path. The APA Minority Fellowship Program funds doctoral and postdoctoral training for clinicians committed to underserved communities. The NBCC Foundation offers fellowships for master's-level counseling students from underrepresented backgrounds. The CSWE Minority Fellowship supports social work doctoral candidates focused on mental health disparities. Smaller programs also fill important niches: the Bespoke Healing Fellowship Program in Chicago centers queer BIPOC graduate students, and the International OCD Foundation runs a Behavioral Therapy Training Institute specifically for BIPOC clinicians treating OCD in communities of color, with its next cohort slated for fall 2026. When evaluating graduate programs, prioritize CACREP-accredited counseling programs or CSWE-accredited social work programs that embed multicultural competency throughout the curriculum rather than limiting it to a single elective.
Resources for BIPOC Therapists and Students Entering the Field
Professional networks, mentorship communities, and funding sources designed specifically for BIPOC mental health professionals can accelerate career development and reduce isolation in a field where representation remains limited. Students and early-career clinicians who connect with these resources often find not only practical support but also a professional home that affirms their cultural identity and clinical approach.
Professional Associations and Affinity Networks
The National Association of Black Counselors serves as a hub for Black mental health professionals, offering a Find a Counselor directory, ongoing community events like Holding Space for Healers, and specialized affinity divisions.1 The Afro Latino Division and Queer Equity and Affirmative Counseling Division create spaces where intersecting identities are centered rather than sidelined.
The Anxiety and Depression Association of America (ADAA) has developed BIPOC-focused Special Interest Groups and training tracks that address minority mental health concerns directly.2 Members can access scholarship opportunities, with BIPOC scholarship recipients featured prominently at the organization's annual conference. These SIGs provide structured peer support alongside continuing education.
Directories and Community Platforms
Our Mental Health Collective operates as both a culturally responsive therapist directory and a community resource hub. Clinicians who identify as Black, African, Asian, Indigenous, Latine, or members of other marginalized communities can create profiles that potential clients browse directly.3 The platform emphasizes culturally affirming care, helping clients find providers who understand their lived experiences without requiring extensive explanation.
Mental Health America's BIPOC Mental Health Resource Center offers educational tools, campaign materials, and advocacy resources aimed at empowering BIPOC individuals.4 While primarily client-facing, the center also provides practitioners with frameworks for community outreach and psychoeducation that resonate with diverse populations.
Scholarships and Training Pathways
Funding remains a persistent barrier for BIPOC students pursuing graduate degrees in counseling or psychology. ADAA's BIPOC scholarship program represents one pipeline, though students should also investigate institutional aid, state-level diversity initiatives, and foundation grants from organizations like the Steve Fund or Boris Lawrence Henson Foundation. Many graduate programs, including clinical mental health counseling online programs, now maintain dedicated recruitment and retention offices for underrepresented students, though the quality and funding of these offices varies considerably.
Connecting early with these resources, ideally during the application process or first year of graduate training, builds a foundation that sustains clinicians through licensure and beyond.
Frequently Asked Questions About BIPOC Therapists
Representation in the mental health workforce affects who seeks care, how they experience it, and whether they stay in treatment. These frequently asked questions address the most common concerns students and prospective clients raise about the BIPOC therapist landscape.
The gap between a diversifying U.S. population and a predominantly white therapist workforce is not closing on its own. As discussed throughout this guide, Black therapists still represent a single-digit share of most licensed mental health disciplines, and metros like Riverside, CA illustrate how large BIPOC communities can be left with startlingly few culturally concordant providers. Pipeline programs, targeted scholarships, and mentorship networks covered in earlier sections are making a difference, but the scale of investment has not yet matched the need.
If you are considering a career in this field, start by exploring accredited counseling, social work, or psychology programs, including pathways such as becoming a mental health counselor. Every new BIPOC clinician who enters practice reshapes the landscape for the communities that need it most.