What you’ll learn in this article…
- AAMFT now permits synchronous telesupervision to count fully toward Approved Supervisor mentoring requirements with no mandatory in-person hours.
- California requires 3,000 supervised experience hours for MFT licensure, one of the highest thresholds in the country.
- Individual MFT supervision typically costs several thousand dollars total, making early budgeting essential for trainees.
- Most states mandate that at least half of your supervision hours come from individual, one-on-one sessions.
Most marriage and family therapy master's programs require 500 to 1,000 hours of direct client contact during training, and virtually all of those hours must be logged under the oversight of a qualified clinical supervisor. That supervised experience is not simply a formality: it is the foundation of your clinical competence, ethical judgment, and readiness for independent licensure. Yet the structure, requirements, and expectations around MFT supervision vary widely. AAMFT sets one set of standards for Approved Supervisor mentoring, while each state imposes its own rules for licensure-track supervision, and many students discover only late in their program that the two systems do not perfectly overlap.
Supervision is also one of the few parts of your education that you will partly control. You choose your supervisor (within certain constraints), negotiate the format, and shape the focus of your sessions. That autonomy comes with responsibility. The difference between transformative supervision and compliance-only check-ins often hinges on how intentionally you approach the relationship and how clearly you understand the rules governing it.
What Is the Difference Between Mentorship and Supervision in MFT?
Clinical supervision and supervision mentoring: two terms that get used interchangeably in casual conversation but describe very different relationships, responsibilities, and purposes within the MFT field. Understanding the distinction early in your training will save you confusion later, especially as you start accumulating hours and thinking about where your career might lead.
Clinical Supervision: The Gatekeeping Function
Clinical supervision is the formal, legally required oversight process that every pre-licensed MFT must complete before earning independent licensure.1 Your clinical supervisor holds direct authority over your casework, your professional development decisions, and ultimately your progression toward licensure. They monitor your clinical skills, evaluate your ethical judgment, and sign off on hours that count toward state LMFT supervision hours requirements.
This evaluative stance is intentional. The supervisor's primary obligation runs not just to you, but to your clients and to the broader standards of the profession.2 State licensing boards and organizational guidelines set the criteria that supervisors must meet, though not all states require the AAMFT Approved Supervisor designation to serve in this role.3 The relationship carries real legal weight: if something goes wrong in a case, the supervisor shares accountability.
Supervision Mentoring: Development at the Meta Level
Supervision mentoring, by contrast, is a process designed for licensed or near-licensed clinicians who are working toward the AAMFT Approved Supervisor designation. The focus shifts entirely. Instead of evaluating a trainee's clinical work with clients, the mentor evaluates a candidate's emerging skills as a supervisor.4
The AAMFT's framework is specific here. A supervision mentor must be an AAMFT Approved Supervisor and a Clinical Fellow with at least 120 post-designation supervision hours. The candidate pursues a minimum of 36 hours of mentoring over at least 18 months, while also providing at least 180 hours of supervision to their own supervisees.4 Completing the AAMFT Fundamentals of Supervision course is also part of the path.5 The mentor's role is developmental rather than gatekeeping: the goal is to give feedback on supervisory practice and ultimately recommend whether the candidate is ready for independent supervision work.
Where the Two Overlap, and Where They Diverge
Both relationships involve a senior clinician guiding someone less experienced, and both carry ethical expectations around confidentiality, professionalism, and feedback. The similarity stops there.
Clinical supervision is tied to documentation, hour logs, and licensure timelines. Supervision mentoring is tied to the development of a specific professional competency (supervising others) that goes beyond direct client care. One relationship focuses on the supervisee's clients; the other focuses on the supervisee's growth as a future supervisor.
Most MFT students will encounter clinical supervision during practicum and internship as a non-negotiable part of their training. Supervision mentoring becomes relevant later, usually after licensure, for those who want to formally credential themselves to supervise the next generation of MFTs. Knowing which type of relationship you are in, and what obligations that creates for both parties, makes the entire process easier to navigate.
AAMFT Supervision Mentoring Requirements Explained
Understanding AAMFT supervision mentoring requirements is essential for MFT trainees who want to know exactly what kind of oversight shapes their clinical development. The AAMFT Approved Supervisor Designation sets clear benchmarks that ensure supervisors are thoroughly trained before they guide the next generation of marriage and family therapists.
To earn the designation, a candidate must first hold AAMFT Clinical Fellow membership.1 From there, the path includes 30 hours of supervision coursework and 36 hours of mentoring under a qualified mentor, all completed over a minimum of 18 months.2 Candidates must also accumulate 180 hours of direct supervision experience with MFT trainees during that period.2 This layered structure means your future supervisor has practiced supervision under expert oversight before ever sitting across from you in a supervision session.
The designation itself is valid for five years.3 To renew, supervisors must complete 20 hours of continuing education, including 3 hours in ethics, 1 hour in cultural competence, and 6 hours in a supervision refresher course.2 These renewal standards exist to keep supervisors current with evolving best practices in clinical training, ethical guidelines, and culturally responsive care.
For trainees, the practical takeaway is straightforward: when your supervisor holds the AAMFT Approved Supervisor Designation, you can be confident they have met rigorous preparation standards. The credit experience pathway also allows supervisors with qualifying backgrounds to demonstrate competence through documented practice rather than following only the traditional coursework route.2
As you progress toward licensure, the quality of supervision you receive directly influences your readiness for independent practice. Students researching best MFT master's programs should pay close attention to whether a program connects trainees with AAMFT Approved Supervisors, since that alignment can streamline your path to counseling licensure after graduation.
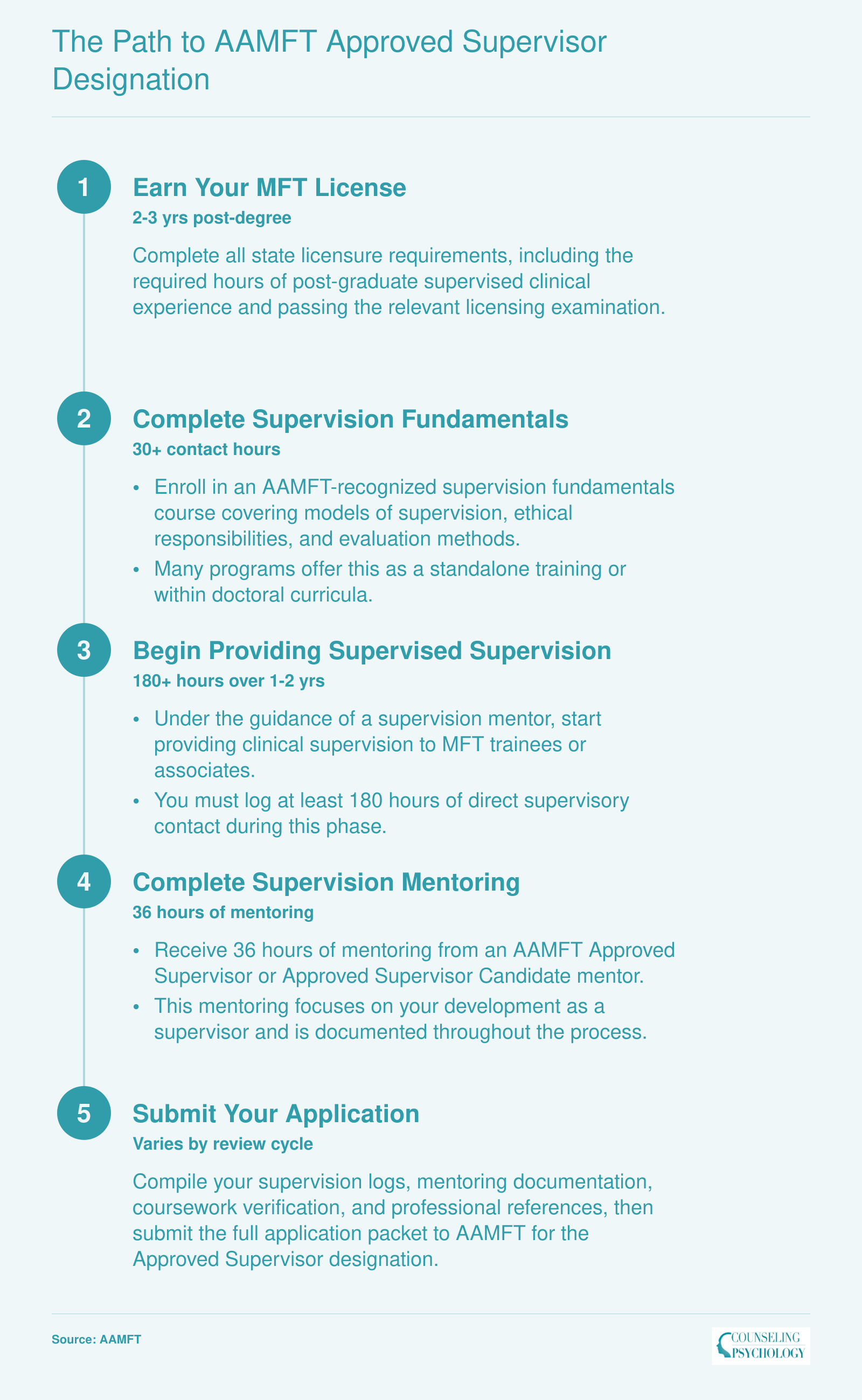
The Path to AAMFT Approved Supervisor Designation
Becoming an AAMFT Approved Supervisor is a multi-year credentialing process that builds on your clinical license. Each phase has specific requirements, and the total timeline typically spans three to five years after licensure. Here is the sequence most candidates follow.
Types of MFT Supervision You'll Experience as a Trainee
Most state licensure boards require that at least half of your total supervision hours come from individual (one-on-one) sessions, with the remainder fulfilled through group supervision. Understanding what each format looks like in practice will help you get the most out of both.
Individual Supervision
Individual supervision pairs you with a single supervisor, typically meeting weekly for about an hour. This is where the deepest clinical work happens. Sessions usually follow a recognizable rhythm: you present a case you are currently managing, your supervisor asks targeted questions about your conceptualization, and together you examine what is working, what is not, and why. Expect feedback on specific clinical skills (joining techniques, circular questioning, reframing) as well as broader developmental conversations about your identity as a therapist. Because of the one-on-one format, there is space to explore personal reactions to clients, countertransference, and ethical gray areas that might feel too vulnerable to raise in a group setting. Individual hours are so central to competency development that licensing boards treat them as non-negotiable: if your jurisdiction requires 100 total supervision hours, plan on at least 50 being individual. For a detailed breakdown of how these requirements vary by state, review our guide to individual supervision hours for MFT licensure.
Group Supervision
Group supervision places a cohort of trainees, usually between three and eight, with one supervisor. Most programs and supervisors cap group size to ensure every trainee has time to present cases and receive substantive feedback. The value here is exposure. You hear cases from populations and settings you may never encounter in your own practicum site. You also practice giving clinical feedback to peers, a skill that carries directly into consultation work later in your career. Group sessions tend to be more structured: a rotating case-presentation schedule, facilitated discussion, and sometimes role-play exercises where one trainee plays the therapist while another plays the client.
Live Observation and Technology-Enhanced Methods
Within both individual and group formats, supervisors often incorporate direct observation. This can take several forms:
- Live observation: Your supervisor watches a session in real time through a one-way mirror or in the room.
- Bug-in-the-ear: A small earpiece lets your supervisor offer brief coaching cues while the session is in progress.
- Video review: You record a session (with proper client consent) and review segments together, pausing to discuss interventions at specific moments.
These methods shift supervision from "what you remember happened" to "what actually happened," giving both you and your supervisor concrete material to work with. Telehealth platforms have made video review especially accessible; many supervisors now use secure portals for trainees to upload and annotate recorded clips between meetings.
What a Typical Session Actually Looks Like
Whether individual or group, most supervision sessions move through four phases. First, you present a case or clinical dilemma with enough context for meaningful discussion. Second, your supervisor provides skill-level feedback, often tying it to a specific theoretical model. Third, the conversation turns to ethical considerations: informed consent, confidentiality boundaries, cultural responsiveness, or mandated reporting obligations that may have surfaced. Finally, you set concrete goals for the next week, such as trying a new intervention, revisiting a treatment plan, or completing specific documentation. Bringing a written agenda or case notes keeps these sessions focused and ensures you leave with actionable next steps rather than vague impressions.
Questions to Ask Yourself
How to Choose an AAMFT Approved Supervisor Mentor
The pool of AAMFT Approved Supervisors has expanded significantly with the rise of telehealth supervision, which means trainees now have more options than ever, but also more variation in style, fit, and quality to sort through. Choosing well early in your post-degree hours can shorten your path to licensure and shape the clinician you become.
Where to Find Approved Supervisors
AAMFT maintains an Approved Supervisor Search tool organized by area. One important caveat: the full directory is accessible only to AAMFT members, and supervisors must opt in to appear, so the public-facing results are not exhaustive.1 Supplement the search with referrals from your graduate program's clinical training office, alumni networks, and your state association. If you are in Texas, the Behavioral Health Executive Council also offers a Find a Supervisor tool that pulls from state-licensed supervisors, surfacing qualified clinicians who hold state supervisor credentials even if they are not AAMFT Approved.
Before your first conversation, verify the credential is current. AAMFT's Approved Supervisor designation is governed by the 2023 Designation Standards and Responsibilities Handbook, and supervisors are required to complete ongoing supervision training to maintain the title.2 A quick check on the directory plus your state board's license lookup confirms both pieces.
Questions to Ask in a Screening Call
Treat the initial meeting like a mutual interview. A focused 30-minute call should cover:
- Supervision philosophy and model: What systemic or relational frameworks guide their work, and how do they structure sessions (live observation, recorded review, case presentation)?3
- Population and setting experience: Have they supervised trainees working with your client population, whether that is couples, adolescents, trauma, or a specific cultural community?
- Availability and format: What is their typical caseload of supervisees, scheduling flexibility, and whether telehealth supervision is offered?
- Feedback style: Do they lean directive or collaborative, and how do they deliver formal evaluations?
- Rupture and repair: How have they handled disagreements or impasses with past supervisees?
Evaluating Fit and Logistics
Beyond credentials, weigh theoretical orientation alignment, cultural responsiveness, and whether they actively support your career direction, whether that is private practice, community mental health, or an academic track. Trainees interested in working across cultural contexts may find it valuable to explore multicultural counseling competencies as part of this evaluation. A supervisor who builds on your strengths rather than reshaping you into their model tends to produce more durable clinical growth.3
Clarify the business side in writing before you start: hourly fee, cancellation policy, expected contract length, documentation responsibilities, and what happens if either party wants to end the arrangement. A clear supervision contract prevents most disputes before they begin.
State-Specific Considerations: MFT Supervision in California and Beyond
California sets a national benchmark for rigor in marriage and family therapy supervision. Its 3,000-hour total experience requirement is among the highest in the country, with distinct rules that shape how aspiring MFTs navigate their pre-licensure journey.
California's Supervised Experience Requirements
Under California BBS regulations, MFT trainees must complete 3,000 supervised hours over a minimum of 104 weeks.1 At least 1,750 hours must be direct counseling, and 500 of those must involve couples, families, or children. No more than 1,250 hours can come from non-clinical activities.3 Trainees must register as an Associate MFT (AMFT) before accruing post-degree hours, though a 90-day grace period allows for immediate post-graduation experience.1 Supervision must occur with a licensed LMFT, LCSW, LPCC, psychologist, or board-certified psychiatrist who has completed a state-mandated 15-hour supervision training.4 The required 100 supervision hours must include at least 50 of individual supervision, aligning closely with AAMFT's standard recommendations.
Where California Goes Beyond AAMFT Guidelines
While AAMFT emphasizes rigorous supervision, California's regulations are stricter in several key areas. The 3,000-hour total far exceeds the 1,000 to 2,000 hours common in many states. The 500-hour couples, families, and children minimum is a unique California requirement not mirrored in AAMFT's general standards.1 Most critically, holding an AAMFT Approved Supervisor credential alone does not satisfy California's supervisor qualifications: state-specific training and licensure are mandatory. The AMFT registration process adds another layer of oversight absent from AAMFT membership guidelines. Students exploring accredited MFT programs online should verify that their chosen program prepares them for these California-specific benchmarks.
State Landscape: New York and Texas
Other states demonstrate the diversity of supervision rules. New York requires 2,000 hours of supervised experience, with supervisors needing to be licensed in a qualifying profession and complete approved training. Texas also demands 3,000 hours but splits them differently, allowing more flexibility in non-clinical activities. Hours distribution, supervisor eligibility, and registration processes vary widely, so students should always consult their own state licensing board early in training.
Telehealth and Technology in MFT Supervision Mentoring
As of 2025, AAMFT permits synchronous telesupervision to count fully toward the Approved Supervisor mentoring requirements, with no minimum number of in-person hours mandated at the national level.1 That single policy change has reshaped how trainees and supervisors connect, but the details matter more than the headline.
What AAMFT and COAMFTE Actually Allow
The AAMFT Approved Supervisor Designation Standards Handbook confirms that synchronous video-based supervision is fully creditable toward AS mentoring requirements, provided no stricter state or program rule applies.1 AAMFT does not specify a particular platform, though its Code of Ethics requires confidentiality, security, informed consent, and competence in the technology being used.2 COAMFTE-accredited programs follow the same framework; there is no cap on telesupervision hours at the accreditation level.3 Programs like Florida State University's MFT track reference both the AAMFT Code of Ethics and the AMFTRB Teletherapy and Tele-supervision Guidelines as their governing standards for remote supervision sessions.4
Best Practices for Effective Remote Supervision
Technology access alone does not guarantee quality. Programs such as UMass Global require a secure, private, synchronous video platform for every telesupervision session.5 Beyond the platform choice, a few habits separate productive remote supervision from awkward screen time:
- Structured agendas: Send your case summaries and questions before the session so both parties arrive prepared.
- Screen-sharing for documentation review: Walking through treatment plans, progress notes, or genograms on a shared screen keeps sessions concrete and skills-focused.
- Relational check-ins: Supervisors should open with a brief personal and professional check-in. Relational depth does not happen by accident when a camera mediates the conversation.
- Backup plans: Agree in advance on a phone or alternate platform protocol for when connectivity fails mid-session.
State Rules Can Override National Flexibility
This is where trainees most often get tripped up. Even though AAMFT and COAMFTE allow full telesupervision, individual state licensing boards set their own rules.1 Some states permit 100% video supervision toward licensure hours, while others impose in-person minimums or restrict cross-state telesupervision entirely. Several states require that the supervisor hold a license in the same state where the supervisee or client is located.1 Before committing to a remote supervisor, verify your state board's current telesupervision policy directly. If you are also sorting out how remote supervision hours count toward licensure, the MFT supervision requirements covered elsewhere on the site can help you start that research.
Advantages and Real Challenges
The practical upside is significant. Geographic flexibility means a trainee in a rural area can access a supervisor with niche expertise in trauma-focused MFT or working with military families, someone who may be hundreds of miles away. Trainees interested in building a remote clinical practice long-term may also want to explore what it takes to become a telehealth therapist. Scheduling becomes easier without commute time, and supervision can continue uninterrupted during relocations or travel.
The challenges are equally real. Reduced nonverbal cues on video can make it harder for supervisors to pick up on a trainee's emotional state. Boundary management requires extra attention; conducting supervision from a shared apartment, for example, risks compromising client confidentiality. Technology failures at inconvenient moments can disrupt the flow of a critical case consultation.
None of these challenges are dealbreakers, but they do require intentional planning. Discuss technology expectations, privacy logistics, and a communication protocol during your first session with any remote supervisor. Treating telehealth supervision as a deliberate professional practice, rather than a casual convenience, is the difference between checking a box and genuinely developing your clinical skills.
Costs, Documentation, and Logistics of MFT Supervision
Understanding the financial and administrative side of supervision early will save you headaches later, especially when you are juggling clinical hours, coursework, and licensure paperwork at the same time.
What Supervision Actually Costs
Nationally, individual MFT clinical supervision runs roughly $75 to $200 per hour as of 2025-2026, with a common mid-range landing between $100 and $160.1 Fees are typically pegged to a supervisor's usual clinical hour rate, so expect higher prices in metro markets and from supervisors with specialized credentials.2 In Colorado, for example, individual sessions tend to fall in the $125 to $150 range, while Texas supervisors frequently charge $75 to $150.3
Group supervision is significantly more affordable. Per-person rates generally run $40 to $90 per hour, representing roughly a 40 to 70 percent discount compared to individual sessions.4 A Colorado group session might cost around $65 per person, while Texas rates cluster between $40 and $75. Group size restrictions vary by state board, so confirm that the ratio in your group actually counts toward your required hours.
Sliding scale arrangements are common, though not guaranteed.1 Other creative fee structures exist as well: flat per-session rates, client-fee splits (where a supervisor waives or reduces fees in exchange for a share of the revenue you generate), and bundled packages. Some nonprofit agencies, hospitals, and federally funded training programs cover supervision costs as part of employment, which is worth factoring into your job search as a post-degree associate.
Supervision During Your Program vs. After Graduation
Most accredited MFT programs fold practicum and internship supervision into tuition.5 Once you graduate, however, the financial picture shifts. Associates pursuing licensure typically pay out of pocket for supervision unless an employer provides it. Planning for 12 to 24 months of weekly supervision expenses (sometimes longer, depending on your state) should be part of your financial roadmap before you finish your degree.
What a Supervision Contract Should Cover
A written supervision contract protects both you and your supervisor. Before your first session, make sure the agreement spells out:
- Session frequency and duration: How often you will meet and for how long each session lasts.
- Fees and payment terms: The per-session or hourly rate, accepted payment methods, and whether a sliding scale applies.
- Cancellation and no-show policies: Required notice periods and any fees for missed sessions.
- Emergency contact procedures: How to reach your supervisor between sessions if a client crisis arises.
- Documentation responsibilities: Who maintains session logs, hour tracking forms, and supervisor evaluation records.
- Termination terms: Conditions under which either party may end the supervisory relationship, including notice requirements and transition planning.
If a supervisor hesitates to put these details in writing, treat that as a red flag.
Why Meticulous Record-Keeping Matters
State licensing boards require detailed proof of your supervised experience, and incomplete or disorganized records are one of the most common reasons licensure applications stall. Throughout supervision you should maintain:
- Session logs: Dates, times, topics discussed, and the format (individual vs. group).
- Hour tracking forms: Running totals of direct client contact hours and supervision hours, broken out by category as your state board requires.
- Supervisor evaluations: Periodic written assessments of your clinical competence signed by your supervisor.
Keep both digital and physical copies. If your supervisor leaves the field, relocates, or retires before you apply for licensure, having your own thorough records ensures you are not scrambling to reconstruct years of work. The AMFTRB state licensure comparison chart can help you identify exactly which documentation categories your board will request, so you can build the right tracking system from day one.
Supervision fees can total several thousand dollars over the full licensure journey, so treat them as a core line item in your education budget from day one. Explore every cost-saving avenue available: employer-sponsored supervision, group supervision formats, and programs that bundle supervision into tuition can all cut expenses significantly.
Red Flags, Ethical Boundaries, and Signs of Quality Supervision
Not all supervision experiences are created equal, and the quality of your clinical oversight directly shapes your development as a marriage and family therapist. Learning to recognize both excellence and warning signs early protects your training, your clients, and your professional future. If supervision becomes harmful or unethical, you have both the right and the responsibility to act.
Pros
- Supervisor provides regular, structured feedback tied to specific clinical skills and observable growth areas
- Cultural humility is practiced openly, with the supervisor inviting dialogue about identity, bias, and lived experience
- Clear boundaries around the supervisory relationship are established from the first session and revisited as needed
- Supervisor actively encourages your growing autonomy rather than fostering dependence on their clinical judgment
- Power dynamics are named and addressed directly, creating a space where you feel safe raising concerns
- Supervisor models ethical decision making and walks you through their reasoning on complex cases
- Availability is consistent and predictable, with a clear process for reaching your supervisor between scheduled sessions
Cons
- Dual relationships emerge, such as the supervisor seeking friendship, business partnerships, or romantic involvement
- Trainee concerns about clients, caseload, or the supervisory process itself are dismissed or minimized
- Supervisor availability is erratic, with frequent cancellations and no reliable way to consult on urgent clinical matters
- Feedback lacks structure or specificity, leaving you unsure what you are doing well or where to improve
- You feel pressured to take on cases or use interventions that exceed your current competence level
- Boundary violations occur, including inappropriate self disclosure, favoritism, or breaches of confidentiality
- If supervision becomes harmful, document every concern in writing with dates and specific examples
- Consult a trusted colleague, faculty advisor, or your program director before deciding on next steps
- Understand how to file an ethics complaint with AAMFT or your state licensing board if the situation warrants formal reporting
Common Questions About MFT Supervision and Mentorship
The supervision and mentorship process raises plenty of practical questions, especially for students mapping out timelines, budgets, and state requirements. Below are answers to the questions MFT trainees ask most often, with references to topics covered in more detail throughout this article.
Treating supervision as a box to check versus a deliberate investment in your clinical identity will shape the therapist you become. The guidance throughout this article points to one consistent theme: supervision quality matters as much as quantity. States like California require 3,000 hours of supervised experience, and fees can reach $200 per session, so planning early is not optional.
Start researching potential supervisors now, verify your state board's specific requirements, and build supervision costs into your education budget from day one. The AAMFT Approved Supervisor directory is your first stop for finding qualified mentors, and your state licensing board can clarify any local rules. Take ownership of this process, and supervision becomes the career accelerator it is designed to be.