
What you’ll learn in this article…
- APA accreditation standards set no fixed percentage cap on telehealth practicum hours, requiring competency demonstration instead.
- State psychology boards vary widely: California, Texas, New York, and Florida each enforce different telehealth hour rules post-pandemic.
- Document every session with separate columns for video, phone, in-person contact, client location, and supervisor modality.
- Programs offering dedicated telehealth coursework, HIPAA-compliant platforms, and diverse practicum sites produce the strongest training outcomes.
Telehealth now accounts for a substantial share of supervised clinical contact in doctoral psychology programs, yet the rules governing those hours remain fragmented across at least three separate authorities. APA accreditation standards set competency expectations without imposing a hard percentage cap. Individual state psychology boards, meanwhile, range from fully embracing remote hours to capping them or requiring specific in-person minimums. Internship sites layer on their own policies.
The result is a genuine tension: students gain scheduling flexibility and exposure to underserved populations through telehealth, but a training plan built around remote hours in one state may not satisfy licensure requirements in another. Documentation missteps compound the risk, especially for trainees planning to relocate after graduation.
How Many Practicum Hours Can Be Completed via Telehealth?
What percentage of my clinical training hours can I complete through telehealth, and who actually sets that limit?
The short answer: there is no single universal cap. The APA Commission on Accreditation does not impose a hard percentage limit on telehealth hours for doctoral psychology programs.1 Instead, most programs and training sites have settled on allowing somewhere between 40 and 60 percent of direct contact hours via telehealth. That range emerged from practical considerations about competency development rather than any regulatory mandate.
Where the 40-60% Range Comes From
Since the APA takes a competency-based, modality-neutral approach, accredited programs have flexibility to determine their own telehealth policies.1 The 40-60% threshold reflects a consensus among training directors that students need substantial in-person experience to develop certain skills (physical assessment techniques, group facilitation, crisis intervention in real time) while also gaining proficiency in telehealth delivery. This is a floor-to-ceiling range you will encounter across different programs, not a formal standard.
APA Guidance vs. State Board Rules
The APA's position treats telehealth as an acceptable delivery modality without prescribing specific percentages.1 Accreditation standards focus on whether trainees can demonstrate competency in assessment, intervention, and other core areas, regardless of how those hours were accumulated.
State psychology licensing boards operate differently. Many boards emphasize the supervision structure and clinical setting rather than the service delivery modality itself, meaning they often make no formal distinction between telehealth and in-person hours.3 However, some states have codified specific requirements about supervision arrangements or clinical settings that can indirectly affect how telehealth hours count toward licensure.
The COVID Inflection Point
During the public health emergency, 100% telehealth training was temporarily permitted across the board. Most of those emergency flexibilities were superseded by 2024 as programs returned to standard operations.2 Some states used the pandemic as an opportunity to codify permanent telehealth allowances, while others reverted entirely to pre-pandemic policies. The landscape is genuinely fragmented.
What Cap Actually Matters for You
If you are pursuing licensure in a specific state, that board's requirements trump your program's internal policies. A program might allow 60% telehealth hours, but if your target state has stricter supervision requirements for remote services, you could find yourself short on qualifying hours at licensure time. Students exploring broader career options, such as those considering how to become a mental health counselor, should note that supervision and hour requirements vary across professions as well.
APPIC Match Sites Add Another Layer
APPIC internship sites expect trainees to have a balanced mix of clinical experiences.4 Individual match sites may impose their own telehealth limits independent of both APA accreditation standards and state board rules. Before ranking sites, verify their telehealth policies align with your training goals and licensure plans.
The safest approach: confirm requirements with your target state's licensing board early, then work backward to ensure your program and practicum placements will produce hours that count.
APA Accreditation Standards for Telehealth Training
The American Psychological Association's Commission on Accreditation (CoA) takes a competency-based approach to telehealth in training. Rather than dictating a maximum percentage of hours that may be earned remotely, the Standards of Accreditation ask programs to demonstrate that trainees achieve the required profession-wide and discipline-specific competencies, regardless of the modality in which those hours accrue.1 For program directors, that translates into documentation work: showing how telehealth experiences map onto assessment, intervention, consultation, and ethical-practice competencies. For students, it means the question shifts from "how many remote hours count?" to "can my program show I'm competent across delivery formats?"
What Changed After COVID
During the public health emergency, the CoA issued temporary flexibilities that allowed expanded telehealth use in practicum, internship, and postdoctoral training. The CoA Winter 2024 Update from the Council of Chairs of Training Councils clarified which accommodations remained in effect and which sunset with the emergency.1 The most durable shift was a 2023 update affecting accredited internships and postdoctoral residencies that addressed supervision authorization for telesupervision under specified conditions. The CoA has not, to date, published a numerical telehealth cap, a minimum required proportion, or a single competency benchmark that programs must meet.1
Site Visit Expectations
There is no public CoA policy that automatically flags programs based on a telehealth ratio alone.1 In practice, however, site visitors evaluate whether a program's evidence of competency development is commensurate with its training model. A program leaning heavily on remote hours can satisfy reviewers if its assessment data, supervision records, and case mix demonstrate that trainees can also function in person when the work calls for it. Thin evidence, not the modality itself, is what creates accreditation risk.
Telehealth-Specific Competencies
The 2024 update to the APA Guidelines for the Practice of Telepsychology continues to emphasize competence as the organizing principle.2 Programs are expected to train students in areas distinct to virtual care:
- Informed consent for remote services: addressing jurisdictional issues, emergency protocols, and limits of confidentiality on digital platforms.
- Technology management: secure platforms, encryption, recordkeeping, and contingency plans for technical failure.
- Cultural and contextual considerations: assessing the client's home environment, digital access, and how identity factors shape virtual engagement.
Doctoral vs. Internship and Postdoc Rules
Doctoral programs, internships, and postdoctoral residencies are accredited under related but separate sections of the Standards. The 2023 supervision-authorization update specifically targeted internships and postdoctoral residencies.1 Students should not assume that a rule clarified at one training level applies identically at another, and program handbooks remain the authoritative source for level-specific requirements.
Questions to Ask Yourself
State Psychology Board Telehealth Hour Rules: A Comparison
State psychology boards have moved in noticeably different directions since the pandemic-era flexibilities expired, and what counts as an acceptable supervised hour in one jurisdiction may not transfer cleanly to another. The six states below (California, Texas, New York, Florida, Illinois, and Ohio) account for the bulk of doctoral psychology trainee licensure applications and represent a range of regulatory philosophies, from permissive to highly prescriptive. Treat this table as a starting point: rules shift frequently, board interpretations matter as much as statute text, and you should confirm current requirements directly with the board where you intend to seek licensure before you log a single hour.
Comparison of Telehealth Hour Rules for Doctoral Trainees
| State | Telehealth counts as face-to-face? | Cap on telehealth hours | Phone vs. video | In-person minimum |
|---|---|---|---|---|
| California | Not explicitly addressed in board rules | None specified | Not distinguished in current guidance | None specified |
| Texas | Verify with board | Verify with board | Verify with board | Verify with board |
| New York | Verify with board | Verify with board | Verify with board | Verify with board |
| Florida | Verify with board | Verify with board | Verify with board | Verify with board |
| Illinois | Verify with board | Verify with board | Verify with board | Verify with board |
| Ohio | Verify with board | Verify with board | Verify with board | Verify with board |
Only California is filled in above because that is the jurisdiction for which we have direct board-level confirmation at this writing. The California Board of Psychology permits telehealth for supervised practice, defines the service location by where the patient is sitting (not the trainee), and does not currently impose a percentage cap or carve out a separate rule for phone-only sessions.1 For the other five states, the honest answer is that you need to read the board's most recent telehealth FAQ or supervision rule yourself, because secondhand summaries (including ours) go stale quickly. If you are still weighing whether telehealth delivery fits your long-term career plans, our guide on how to become a telehealth therapist covers the broader credentialing landscape.
Permanent Flexibilities vs. Reverted Rules
A broader pattern to keep in mind: some states formalized pandemic-era telehealth allowances into permanent rule, while others let temporary orders expire and effectively reverted to pre-2020 supervision expectations. If your training spanned 2020 to 2023, hours that were acceptable at the time of accrual may now sit in a gray zone for licensure in a state that rolled back its rules. Document everything contemporaneously, keep your supervisor's attestations on file, and when in doubt, email the board directly and save the reply.
Related Articles
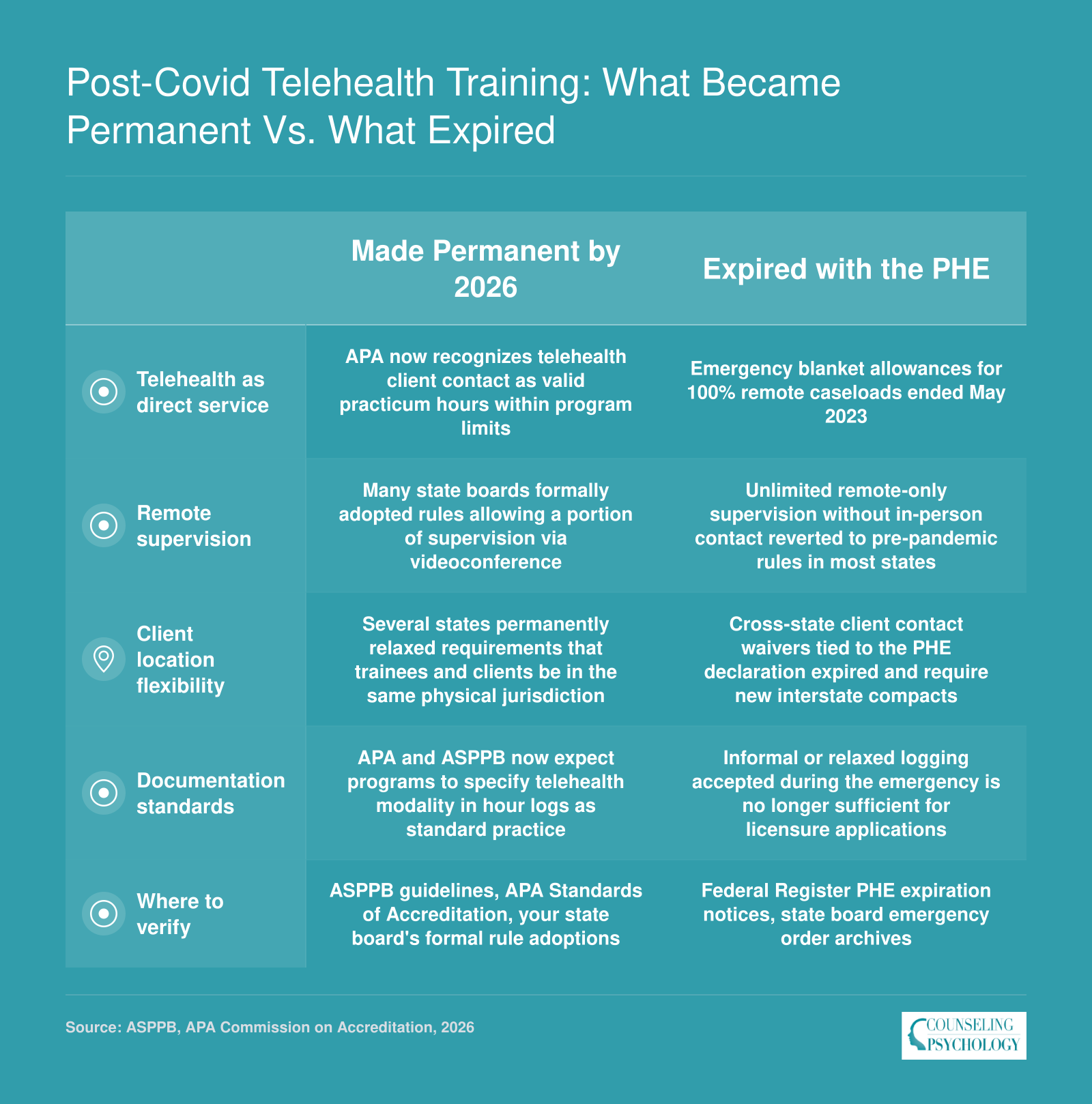
Post-Covid Telehealth Training: What Became Permanent Vs. What Expired
When the federal Public Health Emergency ended in May 2023, many pandemic-era telehealth flexibilities for psychology trainees expired automatically. Since then, some provisions have been formally codified by accrediting bodies and state boards, while others quietly lapsed. Tracking which rules survived requires checking multiple sources: ASPPB and APA policy statements, your state psychology board's adopted rule changes, and professional association newsletters that report on board meeting outcomes.
How to Document Telehealth Clinical Hours for Licensure
Understanding the AAPI's Telehealth Hour Fields
The APPIC Application for Psychology Internships (AAPI) for the 2025-2026 cycle maintains a structure where all direct service hours, both in-person and telehealth, are reported together in the main hour tables.1 However, the form includes separate, specific items designed to capture the telehealth breakdown. You must use these items to indicate how many of your total intervention and assessment hours were delivered via video versus phone.2 No new subcategories were introduced this cycle; the same framework of supplemental telehealth items continues.3 This design makes it essential to track your hours by modality from the start, even though the AAPI's primary tables do not force that distinction.
The Modality Distinction: Video, Phone, and Asynchronous
State psychology boards increasingly differentiate between synchronous video, phone-only, and asynchronous or e-therapy services. While APPIC's current items separate video and phone hours, asynchronous contact, such as text-based therapy or email-based interventions, does not have a dedicated field on the AAPI. For licensure purposes, you must maintain your own logs that clearly categorize these three modalities. Many boards count synchronous video as equivalent to in-person service if supervision and technology standards are met, while phone-only hours may face stricter limits or additional justification. Asynchronous hours are often treated as a distinct category and may not satisfy direct service requirements in some jurisdictions. Separate logging from the outset prevents last-minute scrambling.
Documenting for Multi-State Licensure
If you plan to apply for licensure in more than one state, track your telehealth hours at the most granular level required by any of those target states. Some states demand that you document the client's physical location at the time of service, the supervisor's jurisdiction, and the type of technology used for each session. A consolidated log that captures all these dimensions (modality, date, duration, supervisor present, client location, and any technical interruptions) will satisfy the most stringent board requirements. Avoid the trap of keeping a single "telehealth total" and later trying to reconstruct details; boards view incomplete logs as a red flag.
Common Documentation Errors and How to Avoid Them
Several mistakes frequently lead boards to reject or question telehealth hours:
- Lumping all remote hours together: Using a generic "telehealth" label without separating video, phone, and asynchronous contacts fails to meet board expectations for modality transparency.
- Omitting client location: Many boards need to confirm that the trainee was authorized to provide services in the client's state at the time of the session; missing this data can invalidate hours.
- Inadequate supervision documentation: For telehealth sessions, the log must explicitly show that a qualified supervisor observed or reviewed the work and that the supervisor's license and jurisdiction are recorded.
- Inconsistent totals: When the sum of modality breakdowns does not match the total telehealth hours reported in the main log, boards often return the application for clarification.
- Failing to document telehealth training: Simply listing hours without evidence of formal telehealth training can raise concerns about competency.
Tools for Accurate Tracking
Many doctoral programs provide internal tracking systems, but students frequently supplement these with dedicated platforms like Time2Track or MyPsychTrack. These tools offer telehealth-specific fields for modality, client location, supervisor attestation, and session notes. Students who are still exploring the broader landscape of remote practice may also benefit from reviewing the steps involved in becoming a licensed telehealth therapist. Using a dedicated tracking platform from the beginning of practicum ensures that every dimension is captured automatically, reducing the risk of errors when preparing both the AAPI application and future licensure paperwork.
Telehealth Supervision Requirements for Psychology Trainees
Face-to-face supervision in the same room versus synchronous video supervision from separate locations: both can satisfy doctoral training requirements in 2026, yet the rules governing each format differ sharply across state boards and program policies.
Supervision Modality Is Generally Allowed, With Caveats
Clinical supervision itself can often be conducted via telehealth for psychology trainees. APA accreditation standards formally recognize telesupervision, defined as synchronous audio-video interaction when supervisor and trainee are not in the same facility, and programs are required to maintain a written policy governing its use.1 That policy must address rationale, competency thresholds, risk management, privacy, technology standards, and legal compliance. Montana's psychology board, for example, counts video teleconferencing as equivalent to face-to-face supervision, though audio-only contact is capped at 25 percent of total supervision hours.3
Despite this flexibility, APA standards emphasize substantial in-person supervision experience as a prerequisite.4 Telesupervision is permitted only after trainees demonstrate sufficient competence in conventional face-to-face formats, ensuring foundational skills are established before remote modalities are introduced. Programs typically build this progression into practicum sequences, reserving telesupervision for later rotations or specific circumstances rather than as a default from day one.
How Supervision Format Interacts With Hour Counting
In jurisdictions with restrictive telehealth clinical-hour caps, the modality of supervision can trigger additional scrutiny. Some state boards count hours differently when both the clinical service and the supervision occur remotely, applying the stricter of the two limits. For instance, if a state caps telehealth clinical hours at 50 percent and audio-only supervision at 25 percent, a trainee using both modalities may find the lower threshold governs the entire block of hours. Documentation becomes critical: programs and students must log the supervision format separately from the clinical-service delivery method to demonstrate compliance during licensure application reviews.
Supervisor Qualifications and Training
Supervisors overseeing telehealth training must hold an active license and demonstrate competence in both the clinical activities being supervised and the practice of supervision itself, according to ASPPB guidelines.5 Increasingly, boards and programs expect supervisors to complete formal training in telepsychology ethics, technology security, and remote observation techniques before assuming telesupervision responsibilities. Direct observation methods have expanded beyond in-person presence to include live video monitoring and review of recorded sessions, provided all parties consent and privacy safeguards are maintained.5
ASPPB's Supervision Guidelines serve as a reference framework that many state boards adapt when writing their own rules. Students should cross-check their home state's regulations against the ASPPB baseline, noting any additional requirements for supervisor credentials, trainee-to-supervisor ratios, or mandatory in-person supervision frequency. Trainees who want broader context on the supervision process across disciplines may find it helpful to review LMFT supervision hours requirements for a comparison point. Programs accredited by APA are already held to a floor standard, but state licensure boards retain the authority to impose stricter thresholds that govern post-doctoral practice.
Track every clinical hour with the maximum granularity any state board might require: separate columns for video, phone, and in-person contact, plus client location, supervisor modality, and supervisor attestation. You can always collapse categories later when a board asks for totals, but you cannot reconstruct detail you never recorded.
In-Person Vs. Telehealth Training: Skills and Competency Considerations
APA competency frameworks emphasize that doctoral trainees should develop proficiency across multiple service delivery modalities. Most accredited programs aim for a deliberate mix of in-person and telehealth hours rather than defaulting entirely to one format. This balanced approach reflects the realities of contemporary practice while ensuring students build the full range of clinical skills expected at licensure.
Pros
- Telehealth placements expand access to underserved and rural populations that trainees might never encounter in a traditional clinic setting.
- Students gain firsthand exposure to the service delivery model now used in a significant share of outpatient mental health care nationwide.
- Flexible scheduling allows trainees to fit clinical hours around coursework, reducing burnout and logistical barriers common in practicum semesters.
- Working through telehealth platforms builds technology competency, including HIPAA compliant documentation, virtual rapport building, and digital risk assessment.
- Trainees learn to adapt evidence based interventions for a screen mediated format, a skill increasingly required by employers in 2026.
Cons
- Standardized psychological assessment, particularly with children, often requires in-person administration that telehealth cannot replicate.
- Subtle nonverbal cues such as posture shifts, psychomotor changes, and olfactory indicators are difficult or impossible to observe through a webcam.
- Crisis intervention scenarios involving immediate physical safety (e.g., active self-harm, elopement risk) demand hands-on response skills that remote sessions cannot teach.
- Group therapy facilitation loses important dynamics on screen, including side conversations, seating choices, and real-time interpersonal tension that trainees need to manage.
- Certain populations, including very young children and individuals with severe cognitive impairment, are poorly suited to telehealth, limiting diagnostic exposure.
Choosing a Program Based on Telehealth Clinical Training
What should you look for in a graduate program if telehealth training is a priority for your career?
The answer depends on your target population, licensure state, and long-term practice goals. Not all programs approach telehealth training with equal rigor, and choosing poorly can leave gaps that surface during internship applications or licensing exams. Use a systematic evaluation approach before committing.
Six Evaluation Criteria for Prospective Students
When comparing doctoral or master's programs, assess each against these factors:
- Telehealth hour policy and caps: Does the program set a maximum percentage of practicum hours that can be completed remotely? Programs that align with both APA standards and your target state's board requirements will save you documentation headaches later.
- Variety of telehealth placement sites: A single telehealth-only clinic is limiting. Look for programs partnering with community mental health centers, private practices, hospitals, and school systems that offer remote services.
- Telehealth-specific coursework or competency modules: Standalone electives or integrated units covering telepsychology ethics, crisis management through video platforms, and digital assessment adaptations signal program investment in this modality.
- Supervision modality options: Can supervision occur via secure video when you are placed at a remote site? Synchronous observation capabilities matter for competency verification.
- State board alignment: If you plan to practice in a state with strict telehealth hour limits, confirm the program structures training to meet those thresholds without exceeding them. Understanding how to get a counseling license in your target state is essential to this step.
- Technology platform quality: HIPAA-compliant platforms with integrated documentation, screen sharing for assessment, and reliable connectivity are baseline expectations. Ask what systems the program uses.
School Mental Health Counseling Considerations
Students planning careers in K-12 settings face additional questions. School-based telehealth involves minors, parental consent protocols, and often district-specific platforms that differ from standard clinical software.
During program interviews, ask whether the curriculum includes partnerships with school districts offering telehealth services. Inquire about training on consent procedures for students under 18, confidentiality boundaries when a child is attending sessions from home, and whether practicum sites use platforms like Hazel Health or Daybreak Health that specialize in school mental health delivery.
Warning Signs to Avoid
Programs that rely too heavily on telehealth without guaranteeing adequate in-person assessment training can create serious competency gaps. Psychological testing, behavioral observation in naturalistic settings, and crisis intervention requiring physical presence are skills that cannot develop through video sessions alone.
Internship directors at APPIC-member sites often scrutinize applicants whose practicum logs show minimal face-to-face client contact. Licensing exam content still emphasizes in-person clinical scenarios. A program that markets convenience through all-remote options may leave you underprepared.
Questions to Ask During Program Interviews
Students exploring programs that integrate emerging technology into clinical education, such as AI tools for psychology students, should still prioritize the fundamentals. Come prepared with specific inquiries:
- What percentage of total practicum hours are completed via telehealth versus in person?
- Do you track video-based sessions separately from phone-only sessions in your hour logs?
- What in-person training experiences are guaranteed regardless of placement site availability?
- How do your telehealth hour caps compare to licensing requirements in states where most graduates seek licensure?
Program responses will reveal how thoughtfully they have integrated telehealth into their training model versus treating it as an afterthought or overcorrection from pandemic-era policies.
Frequently Asked Questions About Telehealth Clinical Hours
Telehealth clinical training raises practical questions that vary by program, state, and accreditation body. Below are direct answers to the most common concerns psychology students bring up, with pointers to the relevant sections above for fuller context.