What you’ll learn in this article…
- By 2037, the U.S. will lack nearly 88,000 mental health counselors and 114,000 addiction counselors.
- Only one mental health provider is currently available for every 350 individuals needing care.
- Suicide remains the second leading cause of death for Americans aged 10 to 24.
- Accelerated programs like Baldwin Wallace's 24-month master's are helping close the gap.
For mental health professionals, the workforce shortage presents two conflicting realities: a daily crisis of unmet patient need, and an unprecedented career opportunity. In 2024, more than one in five U.S. adults experienced mental illness, yet only one provider exists for every 350 people needing care.1 Federal projections show the counseling sector will be nearly 88,000 clinicians short by 2037, while addiction counselor deficits top 114,000. That chasm is reshaping licensure pipelines and training models, and it puts newly minted clinicians in a position of leverage. For those weighing counseling vs psychology vs social work, the scarcity is defining hiring landscapes, salary trajectories, and professional identity in 2026.
How Severe Is the Mental Health Workforce Shortage in 2026?
The mental health workforce shortage isn't a distant forecast. It's a daily reality that means Americans are waiting weeks or months for a therapy appointment, if they can find one at all. In 2026, the gap between demand for mental health services and the supply of licensed professionals has grown into a full-blown crisis, with projections showing the problem deepening over the next decade.
The Numbers Behind the Crisis
Federal data paints a stark picture. The U.S. Bureau of Labor Statistics projects that by 2037, the country will face a shortage of nearly 88,000 mental health counselors and 114,000 addiction counselors.1 These aren't just statistics; they represent unfilled positions in schools, community clinics, hospitals, and private practices across the nation. Counseling jobs overall are expected to grow by 25% between 2019 and 2029, far outpacing average job growth, yet training programs aren't producing enough graduates to keep up. The shortfall varies significantly by region, with some states showing the highest need for counselors facing the most acute gaps.
What a Provider-to-Patient Ratio of 1-to-350 Really Means
NAMI reports that for every one mental health provider, there are 350 individuals in need of care.1 In practical terms, this ratio translates into months-long waitlists. Someone reaching out for depression or anxiety support may call five or six practices before finding an available clinician, and even then, the first appointment could be eight weeks out. For those in crisis, such delays can be devastating. The ratio also masks geographic disparities: some areas have ratios closer to 1-to-1,000 or worse, leaving entire communities with almost no access to mental health care.
The Youth Mental Health Emergency
The workforce shortage is especially acute when considering young people. Suicide remains the second leading cause of death among individuals ages 10 to 24, according to NAMI.1 This tragic statistic underscores how urgently accessible counseling services are needed in schools and pediatric settings. Yet school counselor positions go unfilled, and many child and adolescent specialists have waitlists closed to new patients. Understanding which counseling specialties are most in demand can help aspiring clinicians direct their training where the need is greatest. The shortage means that warning signs in children and teens too often go unaddressed until a crisis occurs.
State-Level Recognition of a Workforce Crisis
The severity of the shortage has prompted state organizations to declare emergencies. The Ohio Council of Behavioral Health and Family Service Providers has publicly labeled the situation a "workforce crisis," noting that burnout, low reimbursement rates, and training bottlenecks are hollowing out the pipeline.1 Ohio is not unique; similar alarms are being sounded by provider associations in nearly every state. These declarations reflect a shared understanding that without systemic change, the shortage will continue to undermine community health.
In sum, the mental health workforce shortage in 2026 is not a single problem but a confluence of rising need, lagging workforce development, and structural barriers. For those entering the field, however, it means clear, immediate career demand in nearly every setting.
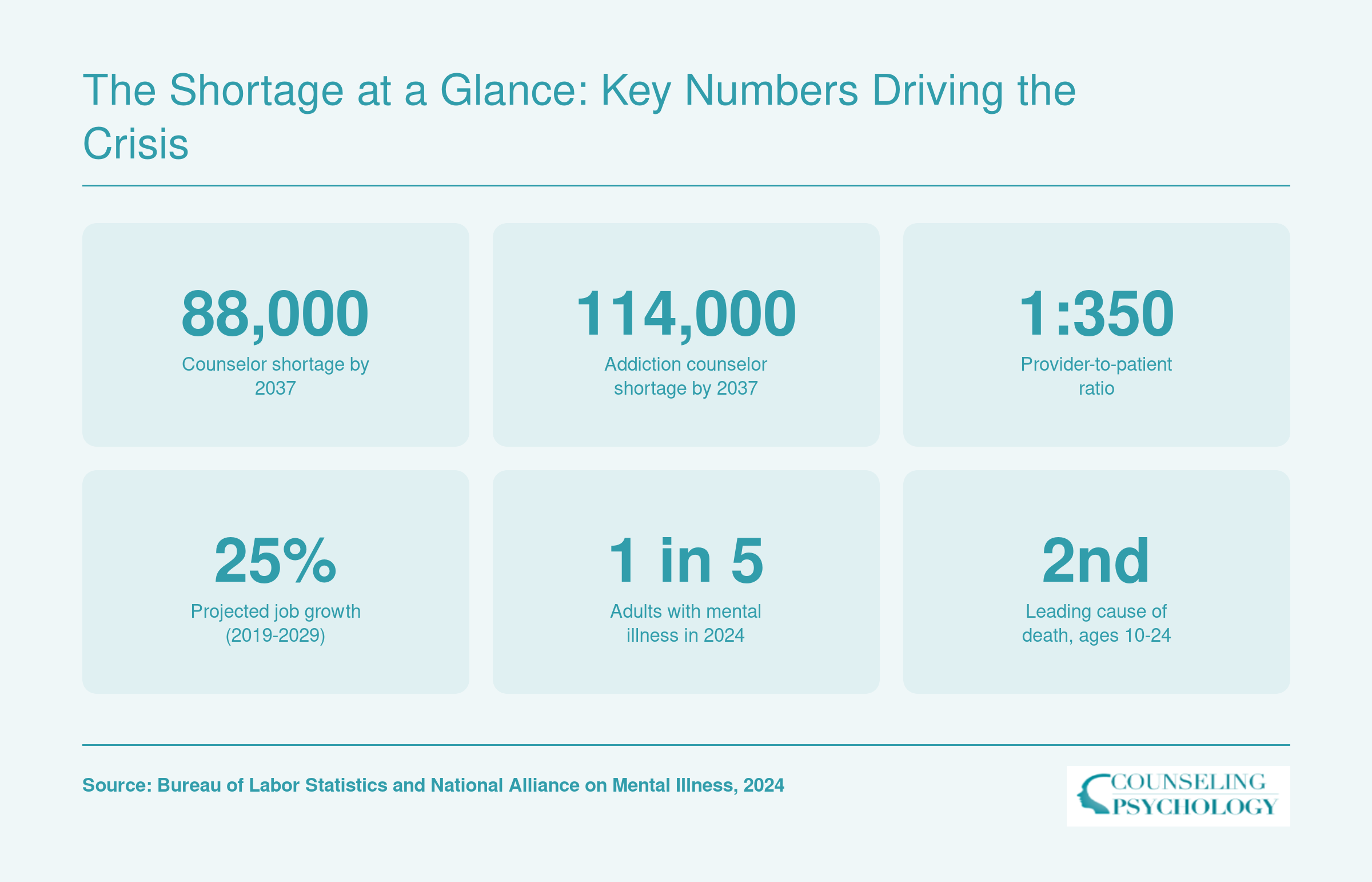
The Shortage at a Glance: Key Numbers Driving the Crisis
The numbers paint a stark picture of the mental health workforce crisis. From provider shortages to rising demand, these figures highlight the urgent need for more clinicians across the country.
Counselor Vs. Social Worker Shortages: A Profession-By-Profession Breakdown
The shortage of mental health professionals is not uniform; it varies dramatically by specific occupation, with some specialties facing more acute gaps than others. Understanding these differences helps you align your education with the areas of greatest need, and opportunity.
Understanding the Shortage Data
Projections from the Bureau of Labor Statistics (BLS) show that many counseling and social work roles are expected to grow much faster than the average for all occupations over the coming decade. While exact growth rates shift with each new projection cycle, the trend is consistent: demand is outpacing supply. The BLS Occupational Outlook Handbook is the best starting point for current, detailed figures, and you can search by SOC code to compare professions directly. Professional associations like the American Mental Health Counselors Association (AMHCA), the National Association of Social Workers (NASW), and the American Psychological Association (APA) regularly publish workforce reports that add context to these broad statistics, highlighting regional and specialty-specific shortages. For a state-level view of where clinicians are needed most, our analysis of states with the highest need for counselors is a useful complement to these national datasets.
Shortages Across Counseling Specializations
Mental health counselors, substance abuse counselors, marriage and family therapists, and psychologists are all experiencing shortfalls, but the intensity and drivers differ. Substance abuse and behavioral disorder counselors, for example, are often cited as having some of the highest projected percentage increases in job openings, driven by the opioid crisis and broader addiction needs. Mental health counselors, particularly licensed clinical mental health counselors (LCMHCs) and licensed professional counselors (LPCs), are in similar demand, with school and community agencies struggling to hire. Marriage and family therapists (MFTs) and clinical psychologists face strong growth as well, though the pipeline for psychologists is constrained by longer training and internship bottlenecks. Students considering that route should weigh the differences between a doctorate degree in psychology and shorter master's-level paths. Many university career centers now publish employment outcomes for their graduates; these numbers often reflect local shortages that can be more dramatic than national averages.
Social Work: Broad Scopes and High Demand
Social workers occupy a unique space in the mental health workforce. The umbrella covers child and family social workers, school social workers, healthcare social workers, and mental health and substance abuse social workers. Each category has its own projection numbers, but collectively the demand is robust. The BLS data tables under "Occupational Projections and Worker Characteristics" allow you to filter by occupation and see projected annual openings, often in the thousands for a single social work category. Because social workers can practice in macro settings (policy, advocacy) as well as clinical roles, the shortage affects not only direct care but also program administration and community interventions. For those mapping out the transition from graduate school to the field, our guide to the social work career journey covers key milestones from MSW to first job. The NASW and its state chapters frequently release reports on vacancy rates, highlighting areas where licensed clinical social workers are hardest to recruit.
Using Reliable Data to Plan Your Path
When weighing a career in counseling versus social work, look past headlines to the nuanced data. Start with the BLS Occupational Outlook Handbook to compare projected growth and typical entry-level education for each SOC code. Then visit professional association websites for workforce reports that break down shortages by region, setting, and specialty. Finally, explore university program pages: many now include employment statistics for recent graduates, sometimes down to the local provider shortage area. This layered approach will give you a realistic picture of where the need is greatest, and where your skills will be most valued.
Related Articles
Where Are the Biggest Gaps? Salary and Employment by State
State-level data pinpoints where the mental health workforce gaps are largest. Social workers earn top median wages in New York ($80,230), Connecticut ($78,820), and Minnesota ($77,100), while counselors see the highest pay in Alaska ($79,220), New Mexico ($70,770), and Oregon ($69,660). Large employment totals in New York and California signal sustained need, even where salaries are moderate, offering reliable entry points for new graduates.
| State | Mental Health Counselors Median Salary | Mental Health Counselors Employment | Mental Health Social Workers Median Salary | Mental Health Social Workers Employment |
|---|---|---|---|---|
| New York | $62,070 | 22,450 | $80,230 | 14,180 |
| Connecticut | $62,960 | 6,470 | $78,820 | 1,350 |
| Minnesota | N/A | N/A | $77,100 | 3,430 |
| California | N/A | N/A | $75,320 | 18,020 |
| District of Columbia | $66,140 | 980 | $72,720 | 640 |
| Oregon | $69,660 | 6,410 | $71,830 | 2,160 |
| New Jersey | $64,710 | 14,640 | $70,420 | 3,140 |
| Hawaii | N/A | N/A | $70,340 | 410 |
| Vermont | N/A | N/A | $69,540 | 370 |
| Washington | $64,220 | 13,150 | $69,060 | 3,490 |
| Maine | N/A | N/A | $67,820 | 1,120 |
| New Mexico | $70,770 | 2,070 | $65,600 | 620 |
| Colorado | N/A | N/A | $65,080 | 1,980 |
| Massachusetts | N/A | N/A | $64,960 | 6,790 |
| New Hampshire | N/A | N/A | $63,810 | 460 |
| Alaska | $79,220 | 1,060 | N/A | N/A |
| North Dakota | $66,450 | 1,180 | N/A | N/A |
| Utah | $65,920 | 4,720 | N/A | N/A |
Rural Vs. Urban: How Location Shapes the Shortage
Geography is the single biggest factor determining whether a community has access to mental health care.
Mental Health Deserts: Rural Shortages by the Numbers
The Health Resources and Services Administration (HRSA) designates vast swaths of the country as Mental Health Professional Shortage Areas, and the map overwhelmingly highlights rural counties. More than three-quarters of rural counties meet the shortage designation, and over 90 percent of U.S. counties have zero practicing psychiatrists. For mental health counselors, the situation is nearly as stark: many rural counties rely on a single provider, if any. In some states, entire regions have no licensed clinical mental health counselor at all. Understanding the mental health counselor shortage by state reveals just how uneven the distribution really is.
When the 1:350 Ratio Plummets
The often-cited national average of one mental health provider for every 350 individuals in need hides severe geographic disparities.1 In rural counties, that ratio can fall to one per 1,000 residents or worse. In frontier and remote areas, such as parts of the Great Plains or Appalachia, people regularly wait six to eight weeks for an appointment and drive over an hour each way. This imbalance means thousands of Americans with depression, anxiety, or substance use disorders go untreated simply because they cannot reach a professional.
Telehealth Bridges the Divide
Telehealth has become a critical tool for closing rural gaps. By delivering therapy and medication management via video, counselors can serve clients who would otherwise have no access, without ever relocating. This shift creates new career pathways: a licensed clinical mental health counselor living in a city can accept patients from rural counties across their state, building a caseload that blends urban and remote clients. Interstate licensure compacts and expanded insurance reimbursement for teletherapy make this model increasingly viable, letting professionals tap into underserved markets from a home office or a co-working space.
Urban Job Markets vs. Rural Realities
Employment data from the Bureau of Labor Statistics shows just how concentrated the workforce is in large metro areas. The New York-Newark-Jersey City region alone employs over 23,700 substance abuse, behavioral disorder, and mental health counselors, with a median salary above $64,900. Los Angeles follows with 23,300 jobs and a median of $58,880. In contrast, the national median salary for these counselors sits closer to $49,000, and in rural counties it often dips below $40,000. The pattern repeats across specialties: mental health and substance abuse social workers in San Francisco earn a median of $78,660, far outpacing the national figure. This urban clustering drives the shortage in remote areas, where community mental health counselor jobs remain unfilled despite overwhelming need. For new graduates, the message is clear: opportunity is everywhere, but the settings, pay, and lifestyle can look wildly different depending on where you choose to practice.
Questions to Ask Yourself
Career Opportunities Amid the Crisis: Settings, Specialties, and Job Growth
The workforce shortage is reshaping where and how mental health professionals work, opening up diverse career paths across settings and specialties. For counselors and social workers entering the field today, demand is not a distant projection: it is an immediate, structural feature of the job market.
High-Demand Practice Settings
Institutional hiring is expanding fastest in settings where mental health needs are most visible. K-12 schools, driven by state mandates for counselor-to-student ratios, now compete aggressively for licensed school counselors and social workers. Community mental health clinics, often the safety net for underserved populations, report persistent vacancies despite steady funding increases. Hospitals and integrated care systems are adding behavioral health consultants to primary care teams, while forensic psychology roles in court clinics, correctional facilities, and juvenile justice settings grow as legal systems divert cases toward treatment. Private practice, once a mid-career goal, is increasingly viable for new licensees thanks to telehealth platforms that eliminate the burden of leasing office space and building a local referral network. Each of these settings offers distinct caseloads, schedules, and reimbursement models, allowing professionals to align their work with their interests and life circumstances. For a broader look at available careers in counseling, the range of options continues to expand.
Specialties Where Need Is Most Acute
Certain specialties face overwhelming demand. Child and adolescent therapy is strained by youth mental health crises, with school districts and pediatric clinics unable to hire fast enough. Substance use disorder counseling is projected to need an additional 114,000 practitioners by 2037 according to the Bureau of Labor Statistics, driven by opioid and polysubstance epidemics.1 Trauma-informed care is now a core expectation in most agencies, creating opportunities for clinicians trained in EMDR, prolonged exposure, and other evidence-based modalities. Forensic psychology continues to expand beyond correctional settings into competency evaluations, custody assessments, and expert witness roles. Marriage and family therapy, often delivered in private practice or agency settings, benefits from strong insurance reimbursement in many states and growing public acceptance. Students exploring their options can compare mft career paths alongside counseling and social work tracks.
Where Employers Are Hiring: Metro-Area Signals
Bureau of Labor Statistics employment data highlights the largest metropolitan areas as hubs for institutional hiring. Cities including New York, Los Angeles, Chicago, Houston, and Philadelphia report the highest absolute numbers of counseling and social work jobs. These metros offer the greatest volume of openings across schools, hospitals, and community agencies, though cost of living and competition vary. For those willing to relocate, these markets provide accelerated career momentum and often offer licensure reciprocity pathways.
Growth That Outpaces Nearly Every Field
The U.S. Bureau of Labor Statistics projects counseling sector jobs will grow by 25% between 2019 and 2029, far exceeding the average for all occupations.1 This trajectory reflects not just population growth but structural gaps that will take years to fill. New graduates in 2026 enter a market where employers actively recruit before licensure is complete, sometimes offering paid supervision and signing bonuses. Those weighing their next move can explore the best jobs for mental health counselors to identify settings that match their training and goals.
Telehealth Opens Faster Paths to Private Practice
Telehealth has transformed the private-practice landscape. Masters-level clinicians can now build a remote caseload with minimal upfront cost, accessing clients across their state through platform-based matching, insurance paneling support, and built-in scheduling. This model circumvents the traditional barrier of years of overhead investment, enabling earlier autonomy and broader geographic reach.
What's Driving the Shortage? Burnout, Training Bottlenecks, and Reimbursement
The mental health workforce shortage isn't caused by a single factor. It's the result of a perfect storm of burnout, training roadblocks, and reimbursement pressures that push clinicians out of the field faster than new ones can enter.
Burnout and Attrition: Why Clinicians Are Leaving
Burnout among mental health professionals has reached alarming levels. A 2024 analysis in JAMA Network Open found therapist burnout rates ranging from 21% to 61%, with an average around 35%.1 Even more concerning, roughly 40% of clinicians experience severe burnout, and certain practice settings see far higher rates:2
- Community mental health: 51% of therapists report burnout.
- Addiction counseling: 50% experience burnout.
- Teletherapy providers: 66% face burnout, likely driven by isolation and high-volume case models.
Key risk factors amplify the problem. Clinicians with high caseloads are 3.2 times more likely to burn out. Less experience doubles the risk, and female therapists have a 1.5 times greater likelihood.2 The result: a 27% jump in turnover once burnout sets in, and 21% of therapists seriously considering leaving the field entirely. A 2025 national survey found that 48% of mental health workers had contemplated quitting their jobs, a staggering figure that underscores the profession's retention crisis.3
Training Bottlenecks: Narrow Pipelines and Long Ladders
The supply of new clinicians cannot keep pace with demand partly because the training pipeline is inherently slow and constrained. Graduate programs in counseling and social work often have limited seats, and faculty shortages in counselor education restrict expansion. Even after completing a master's degree, licensure typically requires two to four years of supervised clinical practice, creating a multi-year lag between enrollment and independent practice. While accelerated programs like Baldwin Wallace University's 24-month clinical mental health counseling track are emerging, the traditional path remains a marathon, not a sprint. This bottleneck means that even as interest in the profession grows, the number of mental health professionals entering the workforce each year falls short of retirements and departures.
Reimbursement and Pay Compression: The Financial Squeeze
Low reimbursement rates from Medicaid and Medicare often fail to cover the true cost of providing care, and slow insurance paneling processes delay clinicians from being paid for their work. In community mental health settings, where salaries are already modest, the financial strain drives many practitioners into private practice or out of the field altogether. Clinical social workers, in particular, face a higher risk of secondary traumatic stress when their pay is lower, according to 2025 data.4 The combination of heavy caseloads and inadequate compensation creates a cycle in which clinicians burn out and leave, further shrinking an already thin workforce.
The Diversity Disconnect
Compounding these issues, the behavioral health workforce does not reflect the racial and ethnic demographics of the communities it serves. This mismatch limits access to culturally responsive care and deepens disparities for communities of color, a gap examined more closely in research on BIPOC therapist availability. Strengthening the diversity pipeline is essential to closing both representation gaps and the overall shortage, yet progress has been slow.
The mental health workforce shortage isn't just about not enough people; it's a vicious cycle where burnout, inadequate reimbursement, and protracted licensure processes each worsen the others. Effective solutions must tackle workforce pipeline, clinician retention, and payment reform simultaneously, not piecemeal, to stabilize the field. Without addressing all three simultaneously, efforts will continue to fall short, as each factor reinforces the others.
Policy Responses and Program Models That Are Working
Addressing the mental health workforce shortage requires more than recruiting new students. It demands systemic policy changes that lower barriers to entry, enhance career flexibility, and incentivize service where it's needed most. Across the country, federal and state initiatives are reshaping the landscape for counselors, social workers, and psychologists, creating concrete opportunities for both new graduates and experienced clinicians. Here are the key programs and policy shifts driving change in 2026.
Federal Loan Repayment and Scholarship Incentives
The National Health Service Corps (NHSC) Loan Repayment Program remains one of the most powerful tools for attracting mental health professionals to underserved areas. Licensed counselors, clinical social workers, and psychologists who commit to serving in designated Health Professional Shortage Areas (HPSAs) can receive substantial loan repayment. For a two-year service commitment, practitioners can qualify for up to $50,000 in loan repayment; extending to three years can increase the award to $75,000. The NHSC Scholarship Program also covers tuition and fees for students in eligible disciplines who agree to work in shortage areas after graduation. Eligibility extends to Licensed Professional Counselors (LPCs), Licensed Clinical Social Workers (LCSWs), and doctoral-level psychologists, making these programs directly applicable to readers of this guide. Many participants find that the financial relief makes working in high-need rural or urban community mental health counselor settings not only possible but professionally rewarding.
Interstate Compacts: Portability for Counselors and Psychologists
Historically, obtaining a new state license to practice across state lines was slow and expensive, limiting therapists' ability to serve clients in multiple states or via telehealth. Two interstate compacts are changing that reality. The Counseling Compact, as of June 2026, includes 39 member jurisdictions, covering a broad swath of the U.S.1 Since its privilege launch on September 30, 2025, six states (Arizona, Georgia, Indiana, Louisiana, Minnesota, and Ohio) are already issuing practice privileges, with 33 more in the implementation pipeline.2 This means LPCs can apply for a single compact privilege that allows them to provide services in any member state, whether in person or through telehealth, without holding that state's license.3 For psychologists, the Psychology Interjurisdictional Compact (PSYPACT) similarly facilitates telepsychology and temporary in-person practice across over 40 participating states. Both compacts eliminate a major administrative hurdle, making it easier for therapists to reach clients in rural and underserved communities and to follow military families or college students across state lines.
Accelerated Training Programs: A Fast Track to Licensure
To speed the pipeline from classroom to clinic, some universities are launching shorter, more intensive degree options. Baldwin Wallace University, for example, began a 24-month master's program in clinical mental health counseling in August 2024. In May 2026, its first cohort walked at commencement, and a new group starts this August. Programs like this trim the typical two- to three-year timeline without sacrificing core training, addressing the immediate need for licensed professional counselors in schools, agencies, and private practices. Other institutions are exploring similar fast-track models, often integrating supervised practicum hours directly into the curriculum to accelerate licensure eligibility. For students, this means entering the workforce sooner and with less total debt, a direct response to both the shortage and the financial barriers many face.
Permanent Telehealth Expansion and State-Level Support
The pandemic-era telehealth waivers demonstrated that remote behavioral health services can be effective and widely accepted. Most states have since made many of these flexibilities permanent. At least 35 states now require insurers to reimburse telehealth visits at parity with in-person care for mental health services, and cross-state practice via compact privileges solidifies the legal framework. This permanence means counselors and social workers can build sustainable telehealth practices, particularly reaching clients in rural counties where mental health services were once nonexistent. Beyond the NHSC, numerous states operate their own loan repayment or forgiveness programs for behavioral health providers who commit to working in medically underserved areas. These programs often offer additional incentives like tax credits, housing stipends, or supervision support, layering onto federal benefits to make careers in shortage areas more attractive. Combined with the compacts and accelerated training slots, the policy environment in 2026 offers concrete, multi-pronged solutions for building the mental health workforce.
Getting Started: Education Paths, Licensure, and Financial Support
Baldwin Wallace University graduated its first cohort from an accelerated 24-month master's program in clinical mental health counseling in May 2026, evidence that streamlined training models can quickly deliver new professionals into a field starved for them. Whether you're drawn to counseling, social work, or marriage and family therapy, the road from classroom to license follows a clear sequence: graduate degree, supervised clinical hours, and a licensing exam. Understanding the milestones up front puts you in control.
Education and Licensure: Two Paths, Two Timelines
Aspiring mental health counselors typically complete a 60-credit master's in clinical mental health counseling online programs, often spanning two to three years, then accrue 2,000 to 4,000 supervised hours before sitting for the National Clinical Mental Health Counseling Examination (NCMHCE) to earn an LPC or LCMHC. Clinical social workers pursue a Master of Social Work (MSW), which takes about two years, and then log roughly 3,000 hours of post-degree supervised practice to qualify for the Association of Social Work Boards (ASWB) exam and LCSW licensure. Both routes lead to independent practice in settings from private offices to hospitals and schools, though the social work degree sometimes opens additional doors in administration and policy. For a detailed breakdown of these credentials, see our guide on the difference between LPC and LCSW.
Accreditation: The Non-Negotiable Quality Mark
Choosing an accredited program isn't just about prestige; it's a licensing prerequisite in most states and ensures your degree meets national standards. Look for CACREP accreditation for counseling programs and CSWE accreditation for social work programs. These bodies confirm that curricula, faculty qualifications, and supervised practicum experiences align with industry standards. Programs without this recognition can force you into extra coursework or delay licensure.
Financial Support That Makes a Difference
Loan repayment programs transform a daunting debt projection into a manageable one. The NHSC Loan Repayment Program awards up to $50,000 for a two-year full-time commitment (40 hours per week) in a qualifying Health Professional Shortage Area, with a half-time option at $25,000.1 Clinical psychologists, LCSWs, LPCs, LMFTs, and psychiatric NPs are all eligible.2 For those targeting substance use disorder treatment, the NHSC SUD Workforce Loan Repayment Program offers up to $100,000 for three years of service.3 Rural practitioners may qualify for the NHSC Rural Community LRP, which likewise provides up to $100,000.4 Beyond federal options, state programs like the California State Loan Repayment Program (serving LCSWs, LMFTs, LPCCs, and psychologists) and Minnesota's Behavioral Health Loan Forgiveness (requiring three to four years of service) add local support.2 Public Service Loan Forgiveness (PSLF) remains a powerful tool for graduates employed by nonprofits or government agencies, forgiving remaining federal loan balances after 120 qualifying payments.
Fast-Track Models: Baldwin Wallace's 24-Month Program
Not every program consumes three or four years. Baldwin Wallace University's 24-month master's in clinical mental health counseling compresses the timeline without sacrificing CACREP-aligned rigor, demonstrating that institutions are responding to the workforce crisis. When evaluating online counseling degree programs, however, look beyond speed: compare supervised practicum hour totals, licensure exam pass rates, and the percentage of graduates who transition directly into clinical roles. These metrics tell you whether the fast track leads where you want to go.
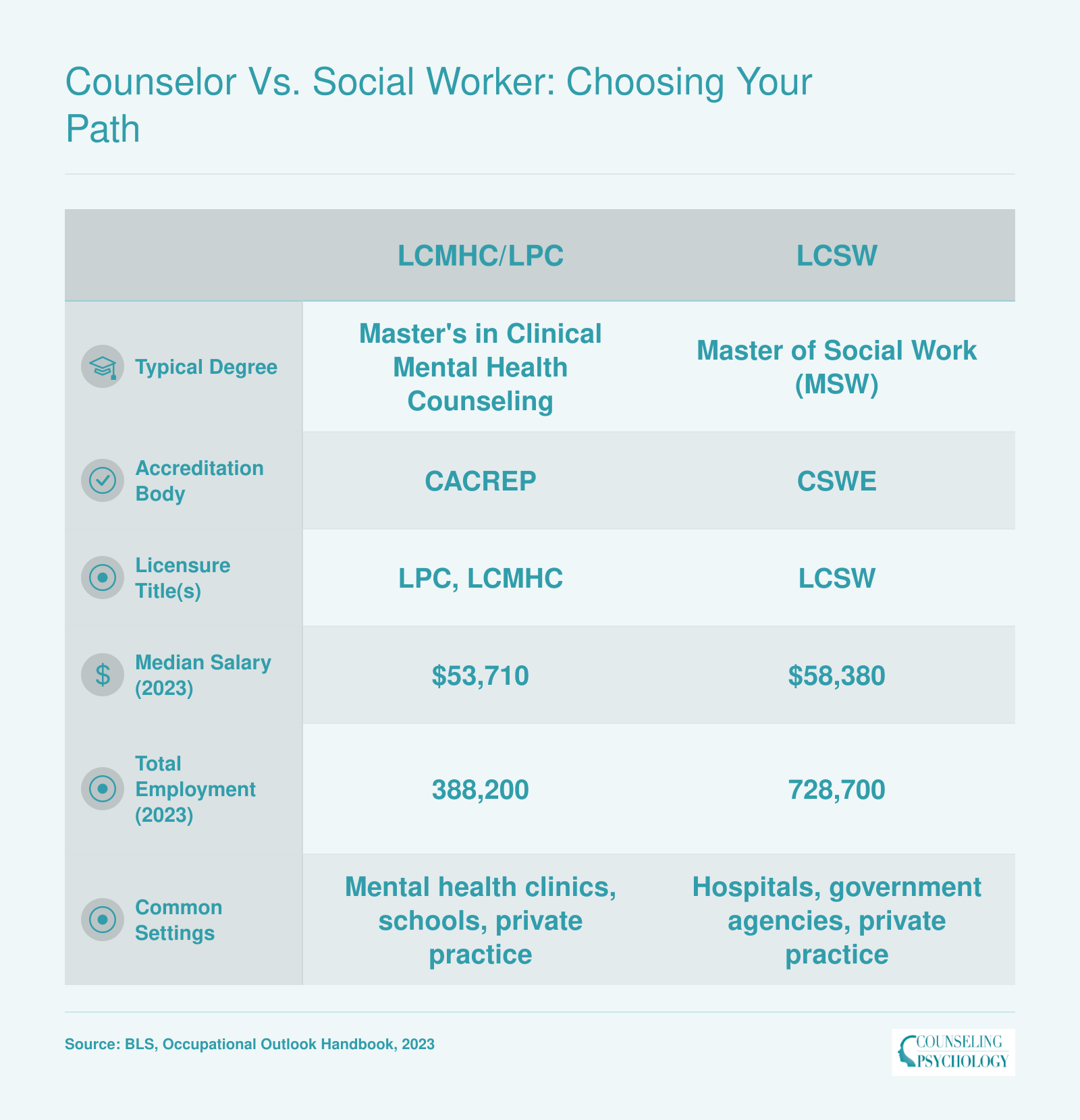
Counselor Vs. Social Worker: Choosing Your Path
If you're weighing a career in clinical mental health, the choice often comes down to becoming a Licensed Professional Counselor (LPC) or Licensed Clinical Social Worker (LCSW). Both paths lead to meaningful work in high demand, but the training, accreditation, and practice settings differ. Here's a side-by-side comparison to help you decide.
Frequently Asked Questions About the Mental Health Workforce Shortage
The mental health workforce shortage dominates conversations in counseling and social work. Below are answers to common questions about the crisis, its causes, and what it means for your career.
The mental health workforce shortage has finally ignited policy reforms that make entering the field more accessible than ever. For communities, this crisis means harmful wait times and limited care; for you, it signals a generation of strong demand. Accelerated programs like the master's at Baldwin Wallace University are cutting training to 24 months, while interstate licensure compacts and loan repayment programs lower financial and geographic barriers.
Your next step is clear: explore accredited programs that match your goals, look to high-need areas such as rural regions, schools, and addiction services where your impact will be immediate, and take the first step toward a career where you are needed from day one. For those still weighing which path to pursue, understanding the most needed psychology specialists can sharpen your focus on where your training will matter most.