What you’ll learn in this article…
- ABA uses the antecedent, behavior, consequence framework to systematically change behavior across clinical and everyday settings.
- All 50 states plus DC now require insurers to cover ABA therapy for autism, though plan details vary widely.
- Hourly ABA therapy rates typically range from $120 to $250, with full programs potentially costing over $62,000 annually.
- Entry-level RBTs can start working in weeks, while the BCBA credential requires a master's degree and supervised fieldwork.
The Behavior Analyst Certification Board reported more than 67,000 active BCBAs worldwide as of early 2025, a figure that has roughly tripled over the past decade. That growth reflects surging demand, but it also raises practical questions for anyone considering the field: which credential level fits your timeline and goals, what the evidence actually supports, and where ABA applies beyond its most visible use case.
Applied behavior analysis is a science of learning and behavior grounded in decades of controlled research. Most people encounter it first through autism intervention, yet the same principles operate in schools, hospitals, corporate training, and substance abuse programs. For those weighing a longer commitment, ABA master's degree jobs span a notably wide range of sectors. The field's rapid expansion has also intensified ethical debates that anyone entering ABA should understand clearly.
The Core Principles of ABA: How Behavior Change Works
How does ABA actually change behavior, and what makes it different from just rewarding kids for good behavior?
The short answer: ABA is built on a precise framework for understanding why behaviors happen and how they can be systematically changed. That framework draws on decades of research, starting with the foundational work of B.F. Skinner on operant conditioning and formalized for clinical practice in a landmark 1968 paper by Baer, Wolf, and Risley, which laid out what "applied" behavioral science should look like in real-world settings.
The A-B-C Model
At the center of ABA is a simple but powerful observation: behavior does not happen in a vacuum. Every behavior is shaped by what comes before it and what follows it. Practitioners call this the Antecedent-Behavior-Consequence model, or A-B-C.
Here is a concrete example a parent will immediately recognize. A child is in a grocery store (the antecedent: a public setting with a desired item in sight). The child throws a tantrum in the candy aisle (the behavior). The parent, wanting to avoid a scene, buys the candy (the consequence). The next trip to the store, the tantrum happens again, and probably sooner.
The consequence reinforced the behavior. That is the A-B-C model in action. ABA practitioners map these chains carefully before recommending any intervention, because changing behavior without understanding its function often backfires.
Reinforcement, Extinction, and What They Actually Mean
A few terms come up constantly in ABA, and they are worth understanding in plain terms.
- Positive reinforcement: Something desirable is added after a behavior, making that behavior more likely to occur again. Praise, a preferred snack, or extra screen time are common examples.
- Negative reinforcement: Something unpleasant is removed after a behavior, which also strengthens the behavior. A child who avoids a difficult task by acting out and is then excused from it has been negatively reinforced.
- Extinction: The reinforcement that was maintaining a behavior is removed, so the behavior gradually fades. Importantly, extinction is not punishment; it is the withdrawal of what was keeping the behavior going.
Understanding the difference between these mechanisms matters because a strategy that works for one child in one context may actively worsen behavior in another. If you are weighing a career in this field, is ABA a good career is a question worth exploring before committing to a credentialing path.
Measurement as a Core Practice
One thing that separates ABA from general behavior management advice is its insistence on data. Practitioners measure the frequency, duration, or intensity of a target behavior before any intervention begins. They continue measuring throughout treatment and after, adjusting their approach based on what the numbers show rather than gut feeling.
This data-driven process is not bureaucratic overhead. It is what allows ABA to catch when a technique is not working early, rather than weeks or months later, and to demonstrate objectively whether a client has made meaningful progress.
What Does an ABA Session Actually Look Like?
If you are considering ABA services for your child or curious about day-to-day work as a behavior interventionist, understanding the session flow and structure is essential. Modern ABA is neither one-size-fits-all nor a rigid drill parade; sessions blend structured teaching with naturalistic play, tailored to the learner's age, goals, and attention span.
The Session Arc: From Hello to Data Review
A typical ABA session runs between one and four hours,1 with younger children often scheduled for 1.5 to 3 hours at a time1 and adolescents working in one to three-hour blocks.2 Intensive early-intervention programs for toddlers and preschoolers may stretch individual sessions to two to six hours when higher weekly dosages are prescribed.3
Most sessions open with a warm-up period lasting 10 to 30 minutes.4 The therapist greets the learner, re-establishes rapport, and reviews the day's target skills. For a young child, this might look like a quick game or choice of preferred toys. For an older learner, it may include a conversation about homework or weekend events. The therapist then spends five to 10 minutes reviewing individualized goals drawn from the learner's Behavior Intervention Plan, a roadmap built after a functional behavior assessment identifies why problem behaviors occur and which replacement skills to teach.4
Next comes the core structured learning block, typically 30 to 60 minutes.4 Here the therapist introduces or practices target skills using methods chosen to match the goal and the learner's learning style. After focused teaching, the session shifts to generalization and wrap-up, a 10 to 20-minute window in which newly taught skills are practiced in less structured contexts such as playground time, snack routines, or pretend play.4 Finally, the therapist spends 15 to 30 minutes collecting and reviewing data, summarizing progress for the supervising behavior analyst and preparing notes for parents.4
Three Core Teaching Methods You Will See
Within that structure, three evidence-based methods dominate:1
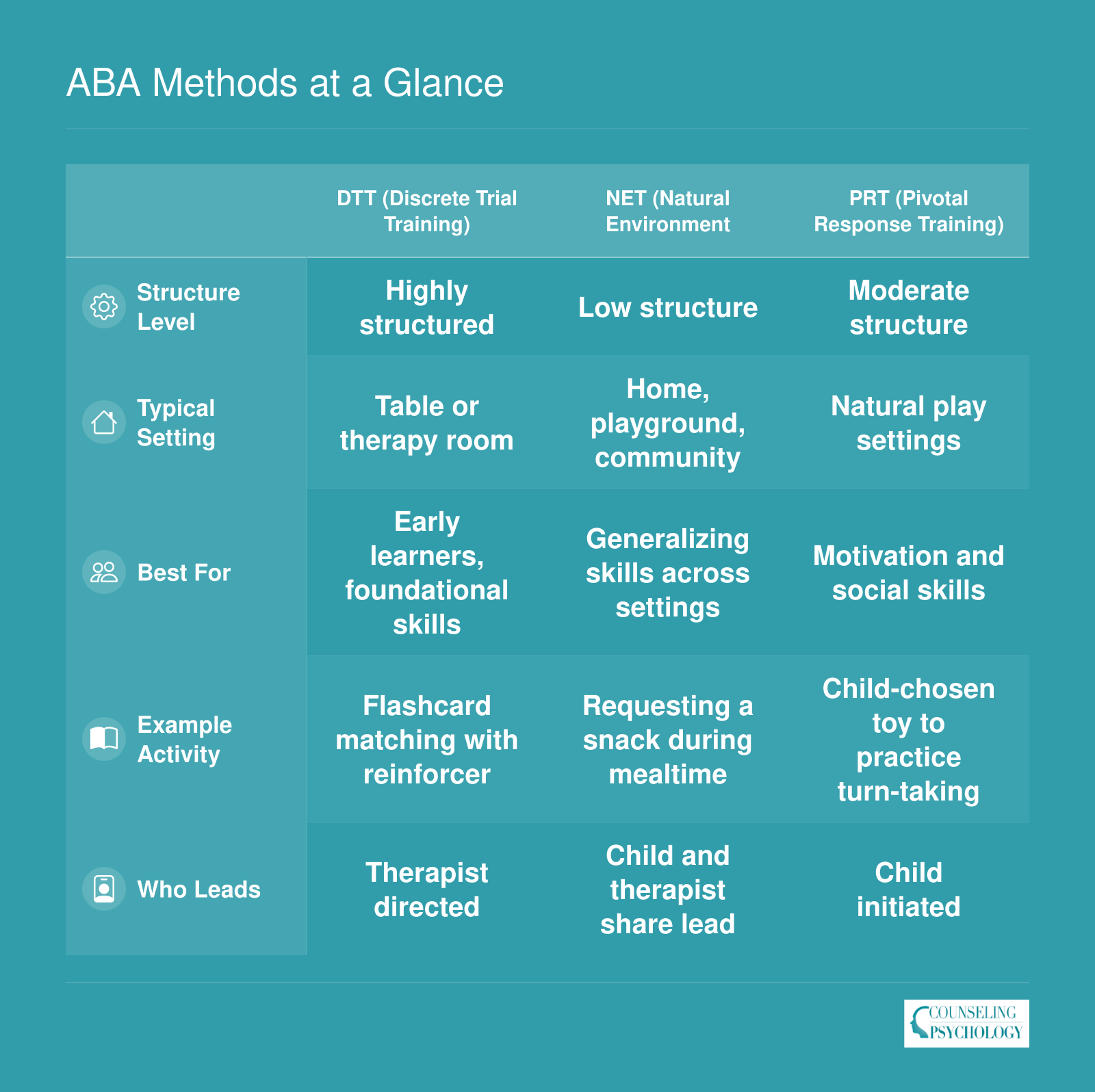
- Discrete Trial Training (DTT): The therapist breaks a skill into small, teachable steps and presents each step in a clear sequence (instruction, learner response, consequence), ideal for teaching foundational skills like matching colors or following one-step directions.
- Natural Environment Teaching (NET): Learning happens during play and daily routines; the therapist follows the child's lead and embeds teaching opportunities into activities the learner already enjoys, strengthening motivation and generalization.
- Pivotal Response Training (PRT): The therapist targets pivotal behaviors such as motivation, self-initiation, and responsiveness to multiple cues, producing broad improvements across many skills rather than teaching one behavior at a time.
Most sessions mix all three methods depending on the moment and the goal.
Intensity, Duration, and the Parent's Role
Program intensity varies by age and need. Toddlers and preschoolers in comprehensive early intervention typically receive 20 to 40 hours of ABA per week,3 while adolescents and young adults working on specific skills may participate five to 20 hours weekly.5 Regardless of intensity, research-backed programs usually run one to three years or longer, because meaningful behavior change takes sustained, consistent practice.
Modern ABA programs also weave in regular parent training sessions. Therapists coach caregivers to use the same prompting, reinforcement, and data strategies at home, ensuring skills transfer beyond the clinic and empowering families to become co-teachers in their child's progress. If you are weighing a career in this field, RBT vs BCBA differences offers a practical breakdown of how these roles divide that day-to-day work.
ABA Methods at a Glance
ABA therapists draw on several structured techniques, each suited to different learners and goals. Here is a side-by-side look at three of the most widely used methods so you can quickly see how they differ in structure, setting, and application.
Applications of ABA: It's Not Only for Autism
ABA is most widely associated with autism spectrum disorder (ASD), and for good reason: decades of research support its effectiveness in building communication, social, and daily living skills in autistic children and adults. But limiting your understanding of ABA to autism misses the broader picture.
Behavior analysts apply the same core principles across a wide range of populations and challenges. Children and adults with intellectual and developmental disabilities (IDD) benefit from ABA-based skill-building programs targeting adaptive behavior, self-care, and vocational readiness. vocational rehabilitation counselors often collaborate with behavior analysts when supporting clients with disabilities in workplace settings.
ABA is also used in:
- Traumatic brain injury (TBI) rehabilitation, where therapists use systematic reinforcement to help patients relearn functional skills.
- Organizational behavior management (OBM), which applies ABA principles to improve workplace performance, safety compliance, and employee productivity.
- Sports psychology and athletic coaching, where behavioral techniques sharpen focus, build consistent routines, and reduce performance anxiety.
- Substance use and addiction treatment, where contingency management, an evidence-based ABA strategy, uses reinforcement to support sobriety.
- School settings, where ABA-informed positive behavior support (PBS) programs reduce disruptive behavior and promote classroom engagement across general education students.
- Gerontology, where behavior analysts help older adults with dementia maintain independence and reduce challenging behaviors.
The common thread across all these applications is the same scientific foundation: observe, measure, intervene, and evaluate. Whether a practitioner is working with a preschooler learning to communicate or a corporate team refining its workflow, the methodology doesn't change, only the target behaviors and the setting do.
This versatility is part of what makes a BCBA career worth considering for people drawn to data-driven helping professions. The credential travels well across sectors, and practitioners rarely find themselves boxed into a single population or environment.
Does ABA Work? What the Research Says
Applied behavior analysis is one of the most extensively researched interventions for autism, with a substantial body of evidence supporting its effectiveness, particularly for young children.
Landmark Studies and Recent Meta-Analyses
The foundation of ABA research includes influential studies such as Lovaas (1987), which reported that 47% of children receiving early intensive behavioral intervention achieved normal intellectual and educational functioning. Later, the Eldevik et al. (2009) meta-analysis confirmed that ABA-based early intervention produces medium to large effects on IQ and adaptive behavior compared to minimal or eclectic treatments.
More recent umbrella reviews and systematic syntheses continue to validate these findings, though they paint a more nuanced picture of effect sizes. A 2023 umbrella review of ABA for autism found small-to-moderate overall effects,1 with specific skill areas varying in responsiveness:
- Cognitive skills: Effect sizes ranged from 0.15 to 0.41, indicating modest but consistent gains.1
- Communication: Expressive language showed effect sizes of 0.46, 0.51, while receptive language reached 0.42, 0.55, often characterized as moderate to large.1
- Socialization: A 2020 meta-analysis reported an effect size of 0.44 for social skills.2
- Adaptive behavior and daily living: Gains were smaller, with adaptive behavior effect sizes between 0.12 and 0.31 and daily living skills at 0.18.1
These numbers reflect that ABA tends to produce meaningful improvements, especially in language and social outcomes, but it is not a uniform solution for all developmental domains.
How Intensity and Duration Shape Outcomes
Research consistently links higher doses of early intervention to larger gains. A landmark finding is that children who receive 25 or more hours of ABA per week for at least one to two years show significantly greater increases in IQ and adaptive functioning than those receiving fewer hours. A 2023 analysis identified that typical effective intensities fall between 10 and 20 hours per week, with higher-intensity programs (15, 20 hours) yielding stronger results than lower-intensity ones (10, 12 hours).1 For children with profound autism, recommendations often range from 30 to 40 hours per week.
A 2024 dose-response analysis confirmed that both greater intensity and longer duration are associated with larger improvements in adaptive behavior.3 This relationship highlights the importance of consistent, comprehensive programming rather than sporadic therapy.
Long-Term Effects and Gaps in the Research
Evidence for long-term maintenance is encouraging but limited. A 10-year follow-up of children who received early intensive behavioral intervention found that cognitive and adaptive gains were largely maintained a decade later.4 However, most high-quality studies focus on outcomes for preschool- and elementary-aged children. Systematic reviews regularly note a thin evidence base for adolescents and adults, with fewer controlled studies examining ABA's impact beyond middle childhood. When older populations are included, the intervention often shifts toward reducing challenging behaviors or building specific life skills, and measures of generalized cognitive improvement are rare.
A Balanced View of the Evidence
While the cumulative research supports ABA as an effective approach, it is critical to acknowledge variability. Effect sizes are generally small to moderate, meaning that not all children show dramatic change, and some skill areas improve more than others. Study quality also varies; many published trials are small, and blinding is difficult to achieve. For adults, the evidence is especially thin, and conclusions should remain cautious. Those considering careers in this field will find it useful to weigh these evidence nuances alongside practical factors like credentialing, which are explored in resources on how to become a BCBA and related pathways. ABA is a powerful early intervention, but it is one piece of a broader support system that must be tailored to individual goals and developmental stages.
How Much Does ABA Therapy Cost, and Will Insurance Cover It?
Hourly rates for ABA therapy run $120 to $250 across most U.S. markets1, with $120 to $150 the typical range cited by industry cost trackers.2 A full program billed at 10 to 40 hours per week translates to roughly $62,400 on the low end and $120,000 to $234,000 for intensive early intervention.3 Initial assessments add another $500 to $2,000 before therapy even begins.3 For families budgeting realistically, expect annual costs of $60,000 to $150,000 for a child receiving a meaningful weekly dose.3
The Insurance Landscape
All 50 states now require some form of autism insurance coverage3, a major shift from a decade ago. The catch: mandates differ sharply in what they actually deliver. Most states impose annual dollar caps, age cutoffs (often ending at 18 or 21), or limits on weekly hours. A handful, including Maryland, New Jersey, Washington, and Indiana, have eliminated dollar caps entirely.4 Private insurance copays typically run $0 to $50 per session once you are in-network3, but finding an in-network BCBA with availability can take months in underserved regions. The applied behavior analysis market faces a documented shortage of credentialed providers in rural and lower-income areas, which compounds the access problem regardless of what your plan covers.
Other Funding Pathways
Families who hit insurance limits or have no commercial coverage have several options:
- Medicaid: Covers medically necessary ABA for children under 21 under the EPSDT benefit, usually with no or minimal cost sharing.3 State Medicaid waivers specifically for autism are available in most states, though waitlists can be long.
- TRICARE: The military's Autism Care Demonstration covers ABA for dependents of active duty, retired, and reserve members.
- School district services: Under IDEA, school-based behavioral support may be written into a child's IEP at no cost to the family, though this is usually less intensive than clinic-based ABA.
- Employer benefits: A growing number of large employers offer behavioral health benefits or autism-specific carve-outs through their health plans or EAPs.
What to Verify Before Signing On
Before committing to a provider, confirm a few non-negotiables: every case should be overseen by a BCBA (not solely RBTs), goals should be individualized to your child after a proper assessment, and the provider should share session data and progress reports with you on a regular cadence. Parent training should be built into the program, not treated as optional.
Red flags worth taking seriously include rigid, cookie-cutter curricula applied to every child, resistance to involving parents in sessions or planning, reluctance to share data, and pressure to commit to 40-hour weeks without a clinical justification tied to your child's assessment.
All 50 US states plus DC now mandate that insurers cover ABA therapy for autism, but coverage details vary significantly by plan. Before starting services, families should verify their specific policy's age limits, hour caps, and in-network provider availability to avoid unexpected out-of-pocket costs.
Ethical Debates and Modern ABA: What's Changed
For decades, ABA has occupied contested ground: lauded by some families and clinicians as transformative, condemned by many autistic self-advocates as compliance training that prioritizes neurotypical behavior over wellbeing. The history is complicated, the lived experiences are real, and the field has begun to reckon with both.
Historical Practices That Caused Harm
ABA was born in the 1960s under Ivar Lovaas, whose early studies on autistic children involved intensive, highly structured programs. Some of those programs used aversive consequences including slaps and, in certain cases, electric shocks intended to suppress self-injurious or aggressive behavior.1 Children were often placed in therapy for 40 hours per week, with goals centered on indistinguishability from neurotypical peers.1
Those practices are no longer used in accredited modern ABA, but their shadow lingers. Autistic adults who experienced those interventions as children describe enduring trauma, and those first-person accounts have driven much of the current critique.
The Core Criticisms From Autistic Self-Advocates
Autistic self-advocates and disability-rights organizations raise several persistent concerns:2
- Compliance-focused goals: Critics argue that traditional ABA emphasizes obedience and conformity (sitting still, making eye contact, responding to instructions) rather than meaningful skill-building or quality of life.
- Suppression of stimming: Repetitive behaviors that help autistic people self-regulate have historically been targeted for extinction, framed as maladaptive rather than functional.
- Normalization over autonomy: The goal of becoming "indistinguishable from peers" communicates that being autistic is inherently a problem to be solved, rather than a neurological difference deserving of accommodation and respect.
- Historical use of aversives: Even though punishment-based procedures are now prohibited, the fact that they were once standard practice raises questions about the field's ethical foundation.
These critiques are not fringe opinions. They reflect the experiences of people who lived through the interventions, and they demand a response from practitioners and families alike.
How the Field Has Responded
Over the past decade, ABA as a discipline has shifted, though not uniformly or fast enough for all stakeholders. Key changes include:
- Assent-based practice: Modern protocols emphasize the child's right to say no. Therapists are trained to read body language, offer choices, and pause or modify tasks if the child signals distress.1
- Trauma-informed approaches: Recognizing that some clients have experienced prior harm, clinicians now incorporate strategies to build trust, avoid triggering environments, and prioritize emotional safety.3
- Neurodiversity-affirming goal-setting: Rather than targeting eye contact or quiet hands by default, best-practice ABA asks whether a behavior actually interferes with the child's wellbeing or access to meaningful activities. Self-stimulatory behaviors that serve a regulatory function are increasingly left alone.
- Ethics code updates: The Behavior Analyst Certification Board has revised its behavior analyst ethics code to explicitly require individualized assessment, positive reinforcement as the primary tool, and respect for client dignity and autonomy.4
Modern naturalistic developmental behavioral interventions like Pivotal Response Treatment and the Early Start Denver Model embed ABA principles in play-based, child-led contexts rather than rigid table work.1 Punishment procedures are not used in contemporary evidence-based ABA.4
Distinguishing Past From Present Without Dismissing Harm
It is both true that modern ABA does not resemble the Lovaas model of the 1970s and true that some practitioners today still employ outdated, compliance-driven methods. Accreditation and ethics codes set a floor, not a ceiling. Families must actively vet providers, and the burden should not fall entirely on parents to identify red flags.
Respect for lived experience means acknowledging that harm was done and that some autistic adults will never see ABA as redeemable, no matter the reforms. That perspective is valid and grounded in history.
Questions to Ask a Prospective ABA Provider
Before enrolling your child, interview the BCBA and ask:
- How do you determine which behaviors to target? Do you assess whether a behavior is harmful or simply non-conforming?
- What is your stance on stimming? Under what circumstances, if any, would you work to reduce it?
- How do you incorporate my child's preferences and assent into sessions? What happens if they refuse a task?
- Do you use any form of punishment or aversive consequence? (The answer should be no.)
- How do you measure success? Is the goal skill acquisition, independence, and quality of life, or is it indistinguishability?
- Are you familiar with neurodiversity-affirming practices, and how do you apply them?
A provider who becomes defensive, dismisses autistic voices, or cannot articulate a clear assent protocol is not practicing modern, ethical ABA. Trust your instincts and prioritize your child's emotional safety alongside their learning goals.
Questions to Ask Yourself
Careers in ABA: Roles, Credentials, and How to Get Started
You can enter ABA through a short technician training that gets you working in weeks, or commit to a graduate-level path that takes years but unlocks clinical authority and higher pay. Both routes are valid, and many BCBAs start as RBTs while finishing school. If you are weighing the two roles side by side, a close look at the RBT vs BCBA career ladder can clarify which entry point fits your timeline and goals.
The Three-Tier Credential Ladder
The Behavior Analyst Certification Board (BACB) oversees three stacked credentials, each with its own scope of practice.
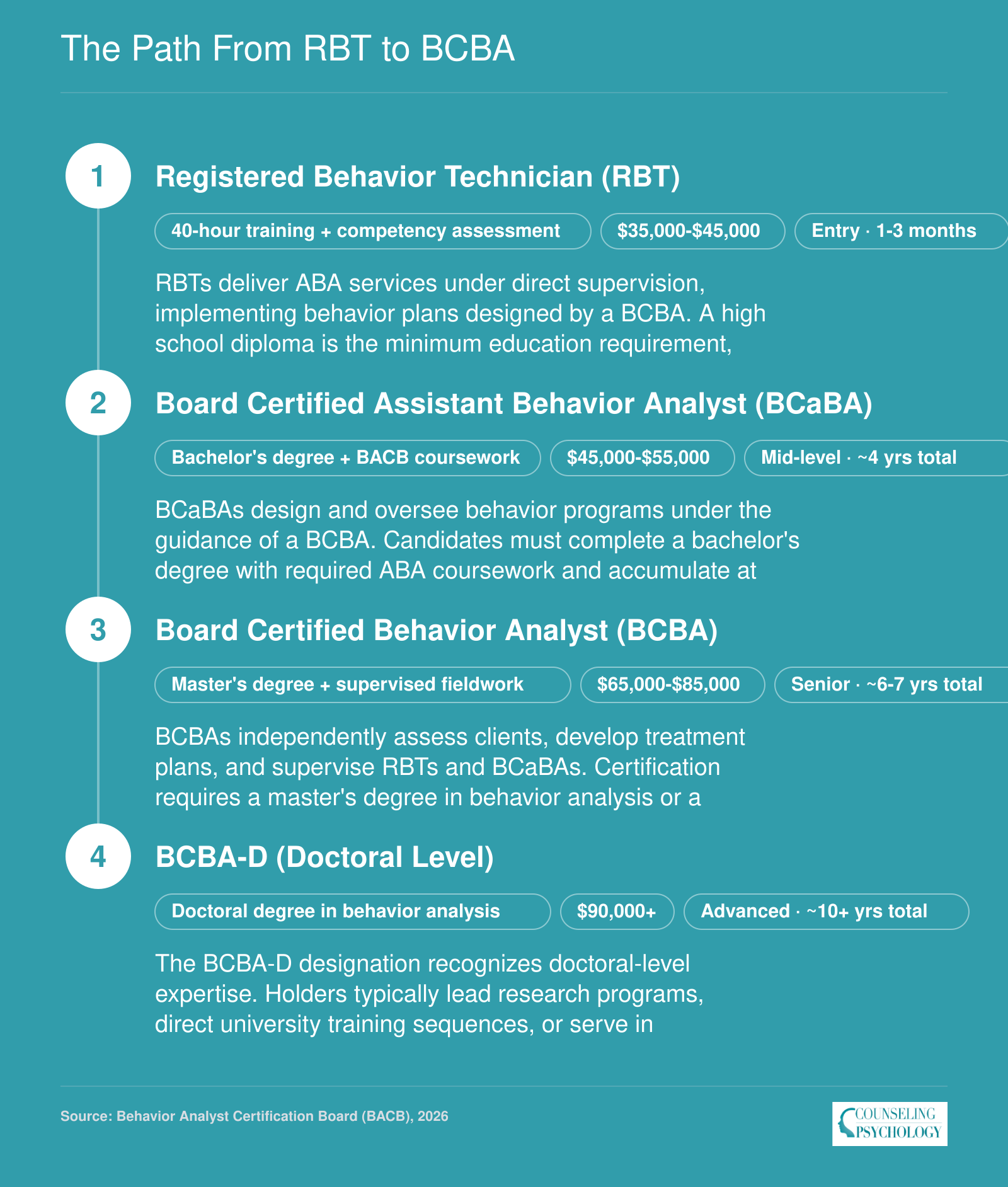
- Registered Behavior Technician (RBT): Requires a high school diploma, a 40-hour training course, a competency assessment, and a criminal background check. Most candidates are credentialed within 2 to 4 months. RBTs deliver direct therapy under supervision.
- Board Certified Assistant Behavior Analyst (BCaBA): Requires a bachelor's degree, BACB-approved coursework, and supervised fieldwork. BCaBAs can design portions of treatment plans but must work under a BCBA. Time to credential typically runs 4 to 5 years including undergrad.
- Board Certified Behavior Analyst (BCBA): The clinical lead role. Requires a master's degree, supervised fieldwork, and passing the national exam. Total time-to-credential generally runs 6 to 8 years from the start of college.
The BCBA Path in Detail
The BCBA is the most-searched credential in the field, and the requirements are tightening. Under the BACB's 2027 standards, candidates need a master's degree or higher from an accredited institution, with verified coursework that stays valid for 10 years.1 Fieldwork moves to a 1,500-hour concentrated model, with at least 60 percent of those hours spent on unrestricted activities (assessment, program design, supervision) rather than direct therapy.1 Prospective students researching BCBA degree requirements and 2027 pathways will find that choosing the right master's program early is the single biggest lever for staying on track.
After eligibility, candidates sit for the multiple-choice BCBA Exam,2 aligned to the 6th edition Test Content Outline that took effect January 1, 2025.1 Certification is maintained through continuing education units (CEUs) and recertification every two years.
Emerging Roles and Job Outlook
Doctoral-level analysts (BCBA-D) lead research, university programs, and large clinical organizations. School-based BCBAs support IEP teams and behavior intervention plans, while Organizational Behavior Management (OBM) practitioners apply ABA principles to workplace performance, safety, and training in corporate settings.
Demand has climbed sharply over the past decade, driven by rising autism diagnosis rates, state insurance mandates requiring ABA coverage, and expansion into adjacent populations including adults with developmental disabilities, brain injury rehabilitation, and gerontology. Job postings for BCBAs have consistently outpaced the supply of newly certified analysts, keeping the labor market favorable for credentialed candidates.
The Path From RBT to BCBA
The ABA credentialing ladder offers a clear, step-by-step progression. Each rung adds education, supervised fieldwork, and earning potential, so you can enter the field quickly and advance at your own pace.
ABA Salary Overview: What Behavior Analysts Earn
The Bureau of Labor Statistics does not publish a dedicated category for Board Certified Behavior Analysts (BCBAs). Instead, BCBA roles are spread across several Standard Occupational Classification (SOC) codes depending on the work setting and job title. The two closest matches are "Psychologists, All Other" (which captures many behavior analysts in clinical and research roles) and "Clinical and Counseling Psychologists" (which includes some BCBAs who hold dual credentials or work in broader therapeutic settings). Because of this imperfect mapping, salary ranges for ABA professionals can look different depending on the source. The figures below are drawn from 2024 Occupational Employment and Wage Statistics published by the U.S. Bureau of Labor Statistics. Keep in mind that BCBA-specific salary surveys conducted by the Behavior Analyst Certification Board often report somewhat different medians, because those surveys capture the credential holder population directly rather than relying on broad occupational codes.
| Occupation (SOC Code) | National Employment | 25th Percentile | Median Salary | 75th Percentile | Mean Salary |
|---|---|---|---|---|---|
| Psychologists, All Other (19-3039) | 17,790 | $73,820 | $117,580 | $145,200 | $111,340 |
| Clinical and Counseling Psychologists (19-3033) | 72,190 | $67,470 | $95,830 | $131,510 | $106,850 |
| Psychology Teachers, Postsecondary (25-1066) | 41,610 | $62,290 | $80,330 | $106,640 | $93,530 |
Frequently Asked Questions About ABA
These are some of the most common questions prospective students and families ask about applied behavior analysis. For deeper coverage, refer to the relevant sections earlier in this guide.