
What you’ll learn in this article…
- Only 37 percent of youth firearm injury survivors receive mental health services within six months.
- AB 2247 would mandate free trauma services for youth gun violence survivors up to age 25 in four counties.
- Firearms became the leading cause of death for U.S. children and teens in 2020, surpassing motor vehicles.
- CalVIP and BSCA grants in California expand trauma-informed mental health care for youth affected by gun violence.
Only 37 percent of children and adolescents who survive a firearm injury receive mental health services within six months, according to a 2023 study published in the American Academy of Pediatrics.1 For the remaining 63 percent, the psychological toll, including PTSD, anxiety, and hypervigilance, compounds unchecked.
California logs about 2,000 firearm-related deaths and hospitalizations among youth 25 and under each year, a number unchanged since 2016. Most survivors cycle through emergency rooms without a reliable bridge to ongoing trauma therapy. As Nicole Kravitz-Wirtz of UC Davis puts it, "It's very clear that violence, and gun violence in particular, is salient in young people's lives."
AB 2247 aims to mandate free mental health care for gun violence survivors up to age 25, but its initial pilot covers just four counties. As the legislation advances, mental health professionals preparing for disaster response and community trauma work will need to evaluate their readiness, even as agencies navigate a patchwork of CalVIP, MHSA, and federal grants to fund that care.
The Treatment Gap: Why Most Youth Gun Violence Survivors Go Without Care
Only 37 percent of children and adolescents who survive a firearm injury receive mental health services within six months, according to a 2023 study published in the American Academy of Pediatrics.1 For the remaining 63 percent, the silence after the emergency room often marks the beginning of a prolonged, invisible crisis. In California, where roughly 2,000 youth aged 25 and younger die or are hospitalized from gun-related injuries each year, the treatment gap leaves tens of thousands of young survivors to navigate trauma without professional support.1
A Widening Care Gap After the Emergency Room
When a young person survives a shooting, the physical wound may heal within weeks, but psychological recovery rarely follows such a linear path. The 2023 study highlights that most survivors are discharged with minimal mental health follow-up, despite clear evidence that early intervention can mitigate long-term harm. In California, where youth firearm injuries have held steady since 2016, the system routinely fails to connect survivors with counseling, therapy, or psychiatric care. The result is a cascade of untreated symptoms that often surface months or years later, when school performance drops, relationships fray, or another crisis erupts.
The Hidden Toll of Unresolved Trauma
Research consistently links firearm-related trauma to a cluster of debilitating conditions: post-traumatic stress disorder, anxiety, depression, hypervigilance, sleep disruption, grief, substance use, and suicidal ideation. As Nicole Kravitz-Wirtz, an epidemiologist with the UC Davis Violence Prevention Research Program, notes, "It's very clear that violence, and gun violence in particular, is salient in young people's lives." That salience means survivors frequently relive the event, scanning their environment for threats even in safe spaces. For Jazelle Eastman, an 18-year-old shooting survivor, the hypervigilance is inescapable: "PTSD is so real, I feel like I'm always looking over my shoulder."1 Without treatment, these symptoms compound, eroding a young person's ability to trust, learn, and plan for the future. Gun violence anxiety in adults follows a similarly disruptive pattern, with research documenting how fear and hypervigilance affect daily functioning long after direct exposure ends.
Disparities Magnify the Urgency
The treatment gap is not distributed evenly. In California, Black youth experience a firearm death rate of 24.8 per 100,000, more than seven times the rate for their white peers (3.4 per 100,000).2 Hispanic or Latino youth face a rate of 5.8 per 100,000, while Asian youth have the lowest at 1.5 per 100,000.2 Overall, 78 percent of young firearm victims in the state are Black or Hispanic.1 These communities often confront additional barriers to care, including under-resourced clinics, insurance gaps, and historical mistrust of medical institutions. Nationally, firearms surpassed motor vehicle crashes as the leading cause of death for children and teens in 2020, and for every death, at least two additional young people sustain nonfatal injuries, a ratio that reaches 4.5 nonfatal to fatal among 15-to-19-year-olds.3 In California, an estimated 20,000 adolescents ages 15-17 reported access to a firearm in 2021-2022, a fact that intensifies suicide risk given that one in four California adolescents reported suicidal thoughts and a third of those attempted suicide.4
Closing the Gap Starts with Acknowledging It
Clinicians and policymakers cannot address what they do not measure. The low service-utilization rate reflects not a lack of need but a system fragmented by long wait times, cost, and a complex compensation structure that confuses families. Survivors like Eastman describe applying for help and never hearing back.1 As California's pilot programs begin to take shape under AB 2247, the state has an opportunity to transform how it responds to youth gun violence, starting with universal, trauma-informed mental health care that reaches survivors before symptoms take hold. For mental health professionals considering where counseling specialties are most in demand, trauma-focused work with gun violence survivors represents one of the field's most pressing and underserved areas.
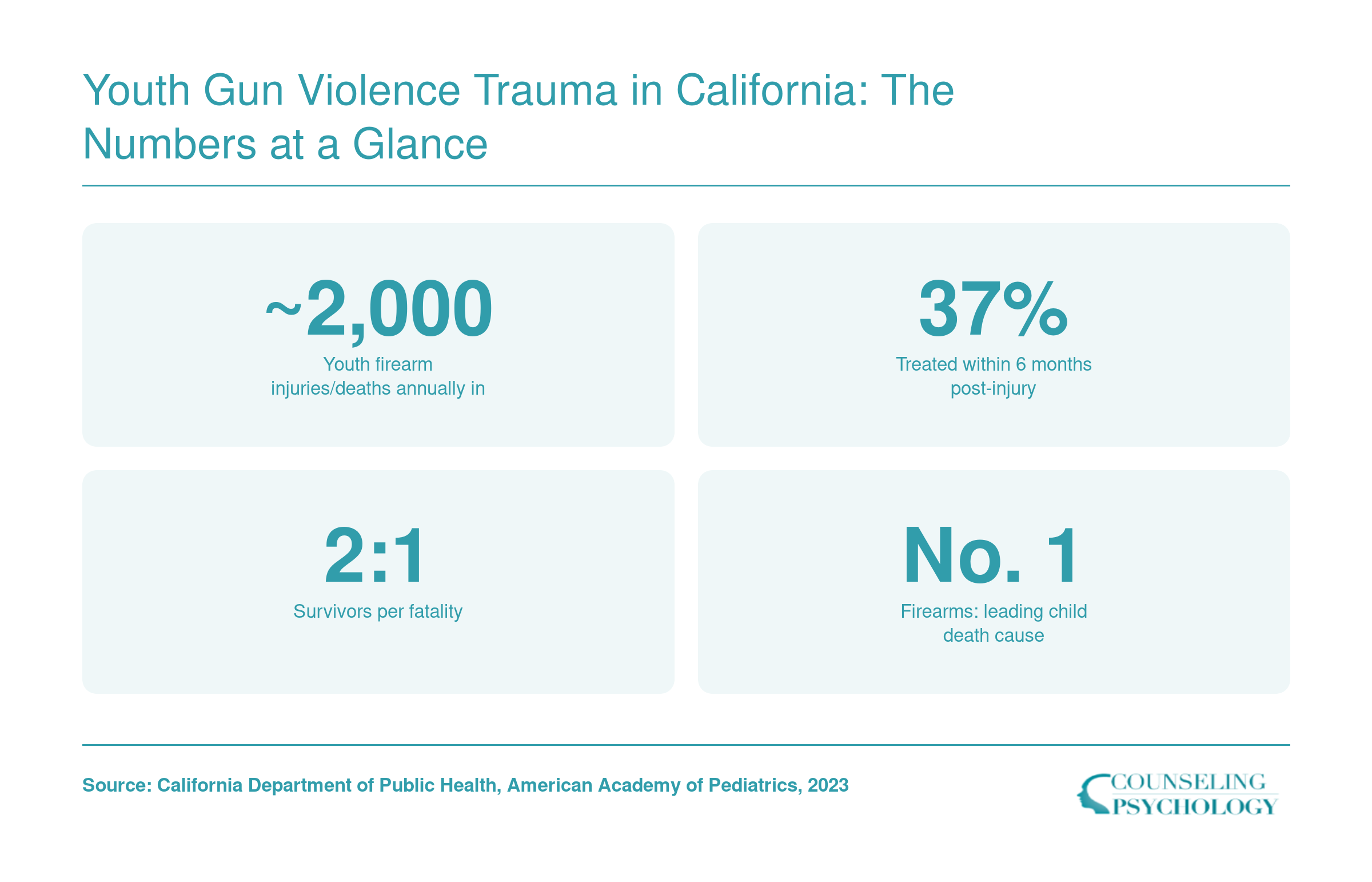
Youth Gun Violence Trauma in California: The Numbers at a Glance
The toll of gun violence on California's youth extends far beyond physical injuries. Each year, about 2,000 young people die or are hospitalized, yet fewer than half receive timely mental health care. Survivors face lasting trauma, and the ripple effects strain families and communities. These numbers capture the scope of the crisis behind AB 2247, legislation aiming to close the treatment gap.
AB 2247 Explained: California's Pilot Program for Youth Survivor Mental Health Services
What exactly would AB 2247 do for youth gun violence survivors in California, and how might it reshape mental health service delivery?
The Bill's Core Mandate
AB 2247, titled the Trauma Healing and Resilience Investment for Victimized and Exposed Youth Act, proposes a landmark requirement: participating counties and the state must provide and fully cover mental health services for young survivors of gun violence, regardless of their insurance status.1 This breaks from the current patchwork where uninsured or underinsured youth often face prohibitive costs and administrative hurdles. The bill aims to guarantee access to trauma-informed care without financial barriers, acknowledging that firearm-related trauma does not wait for insurance approvals.
Pilot Counties: Why These Four?
Alameda, Los Angeles, San Bernardino, and Solano counties form the pilot. Each has a high concentration of youth firearm injuries and fatalities, according to state data, along with existing community-based violence intervention networks that can be leveraged for service delivery. The selection reflects both need and infrastructure, areas where the crisis is acute and where agencies can rapidly stand up coordinated care. The pilot design allows the state to test implementation models, refine reimbursement processes, and gather evidence for potential expansion.
Who Is Eligible?
Free mental health services extend to all gun violence survivors up to age 25 within the four pilot counties.1 This includes those directly injured, eyewitnesses to shootings, and family members of victims, a broad definition that aligns with trauma research showing widespread effects. Covered interventions may range from individual therapy and group counseling to substance use treatment and case management, all grounded in evidence-based, trauma-informed approaches. Importantly, no referral or prior authorization is required, and immigration status does not disqualify a survivor.
Legislative Status as of June 2026
As of mid-June 2026, AB 2247 remains in the early legislative stages.2 The bill was amended on May 18, 2026, and subsequently referred to the Assembly Committees on Health and Judiciary on June 3. It has not yet passed either committee, reached the Assembly floor, or been signed into law. Supporters, including youth advocacy groups and mental health professional associations, are actively lobbying for its advancement, but the timeline for a vote remains uncertain. Mental health professionals should monitor the bill closely, as its enactment would trigger significant operational and training demands. Forensic psychology programs in California may be particularly well positioned to help build the specialized workforce this legislation would require.
Funding and Potential Statewide Scale
The bill establishes the Trauma Healing and Resilience Investment for Victimized and Exposed Youth Fund, with the state required to appropriate money for pilot implementation.1 Funds would flow to county agencies and contracted community-based organizations to cover direct service costs, provider training, and outcome evaluation. While the exact dollar amount has not been finalized, the mechanism allows for annual allocations and federal matching through programs like the Bipartisan Safer Communities Act. If the pilot proves effective at reducing long-term trauma symptoms and improving school engagement, the legislature could scale the model statewide, bringing a permanent, dedicated funding stream for youth gun violence mental health care across California.
Questions to Ask Yourself
California's Broader Funding Landscape: CalVIP, MHWA, and Medi-Cal Reimbursement
California's approach to youth gun violence trauma care is supported by a patchwork of state grants, reimbursement programs, and voter-approved funds. After the immediate crisis, these funding streams determine whether a survivor can access therapy, case management, and long-term recovery. Understanding who holds the purse strings and how to tap them is essential for community-based organizations (CBOs), county agencies, and clinicians.
CalVIP: The Largest Direct Funding Source
The California Violence Intervention and Prevention (CalVIP) grant program is the state's flagship for community-driven gun violence reduction. The current Cohort 5, awarded in 2026, distributed $107 million to 42 grantees1, with a grant period running from April 2026 through June 2029. Funding came from the Gun Violence Prevention and School Safety Fund2 and required no local match.
While CalVIP does not mandate mental health components, many awardees embed trauma-informed counseling into their programs, often through hospital-based violence intervention models. For instance, the Los Angeles County Department of Public Health received $5 million to support hospital-linked street outreach, focused deterrence, and victim services that include mental health care.4 Smaller organizations also benefit: Be Finally Free in Bakersfield was awarded $186,952 as a small-scope CBO.1
Eligibility spans cities, counties, CBOs, and tribal governments.3 The 2025 application deadline passed in August, but future cycles are expected; announcements are posted on the BSCC Submittable portal. Among Cohort 5 grantees, 26 were CBOs, 12 were city agencies, three were counties, and one was a tribal government1, showing that community-level programs are the primary recipients.
Additional State Funding Streams
Beyond CalVIP, several other revenue sources support youth trauma care. The Mental Health Wellness Act (MHWA) provides funds for early intervention, crisis services, and workforce expansion; these dollars often flow through county behavioral health departments and can be subcontracted to CBOs. Medi-Cal, California's Medicaid program, reimburses for trauma-informed individual and group therapy, care coordination, and peer support, provided the provider is enrolled and services meet medical necessity criteria. Additionally, the Mental Health Services Act (Proposition 63) raises about $2 billion annually through a tax on high incomes, and each county decides how to spend its MHSA allocation on prevention, innovation, and direct services. Though not specific to gun violence, these funds frequently address community trauma and youth mental health.
Who Can Apply
The landscape is tiered. CalVIP grants are accessible to CBOs, cities, counties, and tribes directly. MHWA and MHSA funds are generally administered by counties, with community partners eligible for contracts or sub-awards. Medi-Cal reimbursement is available to licensed clinicians and certified clinics, including those in community-based settings. Clinicians who hold clinical psychology degree programs in California may find these roles particularly relevant as workforce demand grows. Individual practitioners cannot typically apply for large state grants, but they can contract with funded agencies or bill Medi-Cal for eligible services. For organizations seeking to launch or expand gun violence trauma programs, starting with CalVIP and county-level MHSA opportunities is the most practical path.
Federal Funding Streams: How BSCA and SAMHSA Dollars Reach California Communities
How do federal programs like the Bipartisan Safer Communities Act actually fund youth gun violence mental health services in California? The path from Capitol Hill to a community counseling center is direct in design but complex in practice, involving block grants, violence intervention programs, and victim compensation funds that clinicians and organizations can tap to close the treatment gap.
The Bipartisan Safer Communities Act (BSCA) and Community Violence Intervention
Passed in 2022, the BSCA represents the most significant federal firearm legislation in decades, channeling billions into school and community mental health. For California, key provisions include:
- School-Based Mental Health Services Grant Program: Funds flow to state education agencies and then to local districts to hire counselors, social workers, and psychologists. These professionals often serve as first responders for youth exposed to community gun violence.
- Community Violence Intervention (CVI) Programs: The California Board of State and Community Corrections (BSCC) administers federal CVI dollars, awarding grants to hospital-based violence intervention programs and street outreach organizations that embed trauma-informed mental health care into their work with young survivors.
- Mental Health Awareness Training Grant: Provides training for educators, law enforcement, and community members to recognize signs of trauma in youth and connect them to services, an essential bridge for firearm injury survivors who often avoid formal care.
SAMHSA's Community Mental Health Block Grant and Set-Asides
The Substance Abuse and Mental Health Services Administration (SAMHSA) Community Mental Health Block Grant (MHBG) allocates flexible dollars to states based on population and need. California receives the largest block grant award nationally, and its Department of Health Care Services (DHCS) disperses these funds through county mental health departments and provider contracts. Important set-asides include:
- Serious Emotional Disturbance (SED) earmark: Requires that a portion of the grant directly serve children and youth with severe mental health needs, which can encompass PTSD and anxiety disorders stemming from gun violence.
- Crisis Services: A 5% set-aside for crisis response systems, which in California funds mobile crisis teams and county-run hotlines that frequently intervene with youth firearm survivors.
- Trauma-Informed Care Integration: California uses block grant funds to train behavioral health staff in evidence-based trauma treatments like Trauma-Focused Cognitive Behavioral Therapy (TF-CBT) and Eye Movement Desensitization and Reprocessing (EMDR), specifically for pediatric populations.
The Chain from Federal Appropriation to Community-Level Service Delivery
Federal dollars flow to California communities through three main channels:
- Formula Grants to State Agencies: MHBG and VOCA (Victims of Crime Act) funds go to DHCS and the California Victim Compensation Board (CalVCB) respectively, which then distribute to counties or reimburse providers for direct services.
- Competitive Federal Grants Awarded Directly to Organizations: Nonprofits, hospitals, and universities can apply directly to SAMHSA, the CDC, or the Department of Justice for programs like Resiliency in Communities After Stress and Trauma (ReCAST) or Hospital-Based Violence Intervention grants, which support mental health for youth affected by gun violence.
- Pass-Through via State-Administered Competitive Programs: For example, the federal CVI dollars augment California's own CalVIP program, which in turn issues requests for proposals to community-based organizations in cities with high rates of firearm assaults.
Grants Specifically Targeting Youth Firearm Injury Survivor Mental Health
Several federal streams explicitly fund mental health services for youth gun violence survivors, though they are often under-deployed because of fragmented application processes and awareness gaps:
- VOCA Victim Compensation: CalVCB reimburses counseling costs for crime victims, including gun violence survivors up to age 25, covering sessions with licensed clinical social workers, MFTs, and psychologists. Providers must register with CalVCB and bill for services.
- CDC Community Violence Prevention Grants: Funded through BSCA, these grants support evidence-based strategies in communities with high firearm injury rates. Many recipients use the dollars to embed mental health clinicians in emergency departments or youth centers.
- Office of Juvenile Justice and Delinquency Prevention (OJJDP) Trauma-Informed Care Grants: These support programs for justice-involved youth, a population disproportionately affected by gun violence, to receive trauma-specific therapy.
For clinicians, the takeaway is that federal funding is available but often requires active engagement. Professionals working in childhood trauma counseling may find particular value in enrolling as VOCA vendors or advocating for local school districts to use BSCA dollars for mental health hiring. Building familiarity with these streams can position a practice or agency to become part of the safety net for young survivors seeking care.
Related Articles
Barriers to Access: Insurance, Trust, Wait Times, and Systemic Gaps
Even when the psychological toll of gun violence is clear, young survivors in California routinely hit a wall when they try to get help. The obstacles fall into three broad categories, each enough to derail recovery on its own.
Financial Hurdles: Uninsured and Underfunded
- Insurance gaps: Many youth lack private coverage, and Medi-Cal eligibility can be delayed or misunderstood, leaving families to front-load costs.
- Victim compensation maze: California's Victim Compensation Board (CalVCB) is meant to cover counseling, but the process is notoriously slow and confusing. Survivor Jazelle Eastman applied twice and never heard back, despite the program's promise to pay for therapy for firearm victims.
- Out-of-pocket costs: Without approved compensation or insurance, copays and session fees quickly become unsustainable, especially in communities where economic strain is already high.
Systemic Bottlenecks: Wait Times and Workforce Gaps
- Clinician shortages: Trauma-specialized therapists remain scarce across the state. High-violence counties like Alameda and San Bernardino report months-long waiting lists for youth services, effectively shutting out survivors during the critical post-injury window when symptoms first emerge.
- Lack of culturally competent care: Many providers are not trained to work with adolescents from communities that experience chronic violence, making sessions feel irrelevant or alienating.
- Referral breakdowns: Emergency departments and pediatric trauma centers often lack direct pathways to mental health follow-up. One multi-state study found that only 37% of children received mental health care within six months after a firearm injury,1 a figure that reflects system fragmentation more than a lack of need.
The Trust Deficit: Engaging Communities in Crisis
For youth who have witnessed or survived shootings, the very institutions that offer help can feel unsafe. Police involvement in hospital responses, mandatory reporting concerns, and a history of over-surveillance in some neighborhoods breed suspicion. Community mental health counselors working in these settings face a particular challenge: building rapport with young clients who associate formal systems with harm. Jazelle Eastman describes the aftermath: 'PTSD is so real, I feel like I'm always looking over my shoulder.' Yet she also notes that 'talking to someone made it a lot better,' a reminder that engagement is possible when services are delivered through trusted community messengers rather than impersonal systems. Building that trust requires time, consistency, and a visible commitment to confidentiality that many current programs lack. The shortage of BIPOC therapists compounds this problem, as clients are far more likely to engage when they see themselves reflected in their provider.
Sure, funding matters. But trust is the real make-or-break for youth survivors of gun violence. Before any therapy sticks, clinicians need to show up inside the community, consistently, culturally, and without judgment. Engagement is not an intake form; it is a relationship built where the young person already stands.
What Clinicians Should Prepare For: Workforce Demand and Evidence-Based Approaches
How can clinicians get ready for the expected surge in youth gun violence trauma cases, and which treatments have the strongest track record?
The Coming Surge in Demand for Trauma-Informed Care
With AB 2247's pilot program aiming to extend no-cost mental health services to gun violence survivors up to age 25, clinicians across California can anticipate a significant increase in referrals. The current gap, where only a minority of child survivors receive timely mental health care, indicates a vast unmet need. Expanding access will require not only more therapists but also practitioners who are specifically prepared to address the complex trauma that follows firearm injuries. Professionals in forensic psychology, clinical counseling, social work, and marriage and family therapy must evaluate their readiness to meet this demand, including their familiarity with youth-specific trauma interventions and their capacity to work within often under-resourced public systems. Understanding types of counselors that work with kids can help practitioners identify where their skills fit most naturally within this expanding service landscape.
Evidence-Based Interventions for Firearm-Related Trauma in Youth
Leading professional guidelines and trauma-focused organizations point to several established treatments for posttraumatic stress in adolescents and young adults. Trauma-Focused Cognitive Behavioral Therapy (TF-CBT) is widely recognized for children and teens, integrating exposure, cognitive processing, and caregiver involvement. Eye Movement Desensitization and Reprocessing (EMDR) and Cognitive Processing Therapy (CPT) are also used with adolescent populations, though their evidence base for firearm-specific trauma is still emerging. Many studies on these modalities have focused on physical abuse, sexual assault, or natural disasters, but the core mechanisms, such as addressing hypervigilance, intrusive memories, and avoidance, are highly relevant to gun violence survivors. Practitioners should seek training and consultation in at least one of these evidence-based models and remain attentive to adaptations for community violence exposure, which often involves chronic, repeated trauma rather than a single incident.
Building Competency and Staying Current
Given the evolving nature of trauma science, clinicians have several avenues to deepen their expertise:
- Review curated resources: The National Child Traumatic Stress Network (NCTSN) offers fact sheets, training materials, and a searchable directory of evidence-based programs, including those specific to violent injury.
- Engage with professional networks: Divisions such as APA Division 56 (Trauma Psychology) and the International Society for Traumatic Stress Studies provide access to webinars, special interest groups, and practitioner forums that address youth violence.
- Monitor the research pipeline: Setting up alerts in journals like *Journal of Traumatic Stress*, *JAMA Pediatrics*, and *Journal of Adolescent Health* can help clinicians stay informed about the latest outcome studies and implementation science relevant to firearm trauma.
- Seek supervision and advanced certification: Participating in structured learning collaboratives or obtaining certification in trauma-focused modalities not only enhances clinical skill but also positions practitioners to meet future state-funded service requirements.
As California moves to close the treatment gap for youth gun violence survivors, a prepared workforce will be the linchpin. Proactive clinicians who invest in trauma-informed training and stay connected to emerging evidence will be best equipped to provide the effective, accessible care that this population urgently needs.
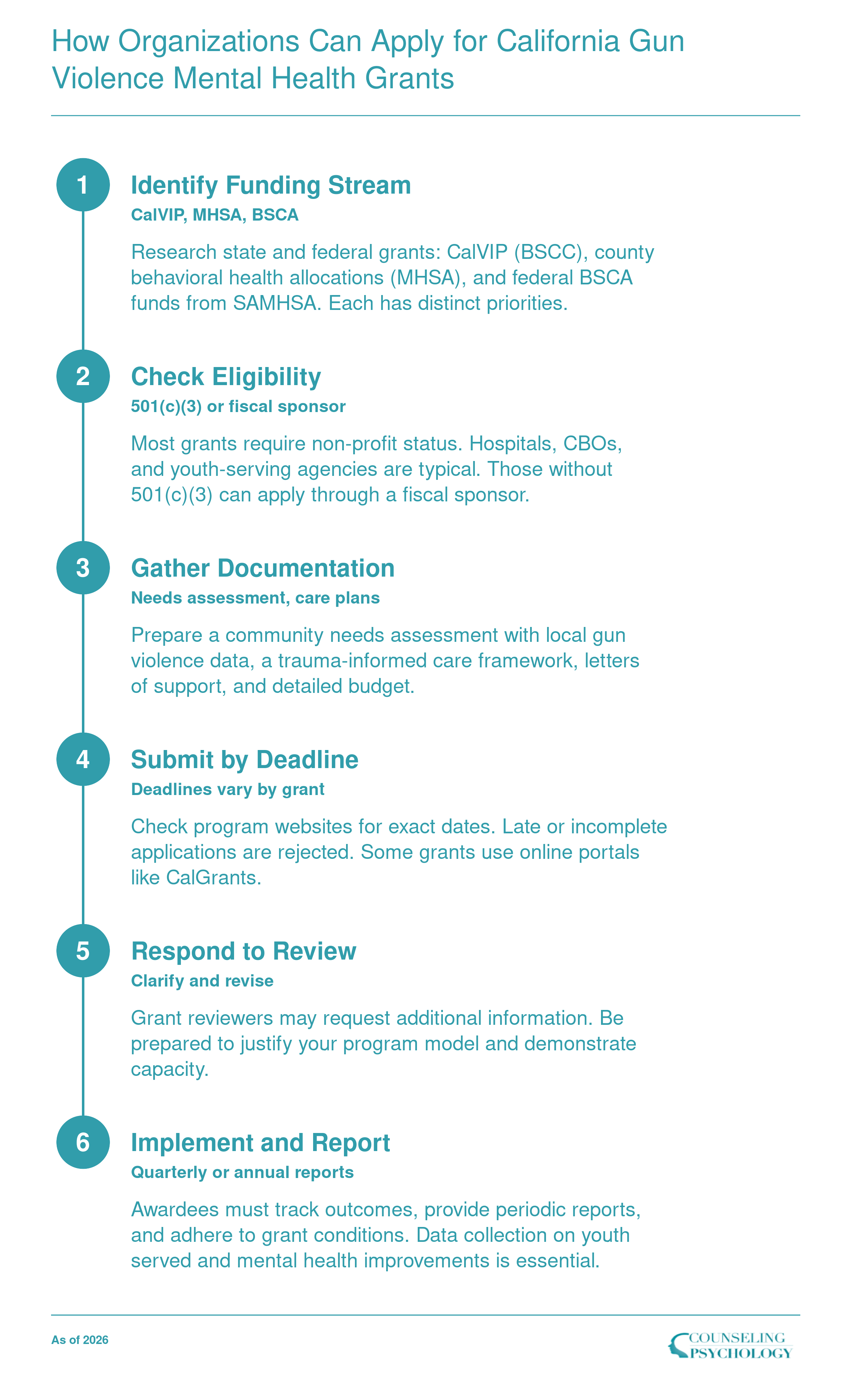
How Organizations Can Apply for California Gun Violence Mental Health Grants
California has multiple funding streams for youth gun violence trauma care, including CalVIP grants administered by the Board of State and Community Corrections (BSCC) and county-level Mental Health Services Act (MHSA) dollars. Applications typically require a clear trauma-informed care model and evidence of community need. Successful proposals often partner with established fiscal sponsors if the organization lacks 501(c)(3) status.
Grant Application Checklist for Community-Based Organizations
Securing funding for youth gun violence trauma services requires a well-prepared application. Use this checklist to gather commonly requested materials for CalVIP, BSCA-funded, and county-level grants.
- Organizational capacity documentationProvide proof of nonprofit status, staff credentials, fiscal policies, and experience serving youth populations.
- Evidence-based program modelDetail your chosen intervention (e.g., trauma-informed cognitive behavioral therapy) and cite supporting research.
- Memoranda of understanding (MOUs) and letters of supportSecure commitments from hospitals, schools, violence intervention programs, and other community partners.
- Data collection and evaluation planDescribe how you will measure client outcomes, such as reduced PTSD symptoms or improved school attendance, and report to funders.
- Budget narrative and detailed line-item budgetJustify all costs, including personnel, training, equipment, and indirect expenses. Show alignment with program activities.
- Grant-specific tailoringFor CalVIP, emphasize violence reduction and community-based strategies. For BSCA funds, coordinate with local education agencies. For county grants, align with local mental health plans.
Frequently Asked Questions About Mental Health Grants for Gun Violence Trauma in California
As California policymakers and communities push to close the mental health treatment gap for youth gun violence survivors, clinicians and organizations face practical questions about funding, legislation, and clinical best practices. This FAQ provides clear answers grounded in current law and evidence to help advocates and providers navigate the evolving landscape.