What you’ll learn in this article…
- Most states require 1 to 6 hours of DV training for licensure, but specialists need far more.
- Modular, asynchronous curriculum designs let organizations train dozens of clinicians without disrupting caseloads.
- Median DV therapist pay hovers near $50,000 despite advanced trauma specialization demands.
Domestic violence service demand has risen sharply over the past decade, yet fewer than half of community mental health agencies report having therapists with formal, specialized training in trauma-informed domestic violence intervention. The gap between caseload growth and clinician readiness creates urgent pressure on training infrastructure.
This article is not a career guide for individual therapists. It focuses on the design and delivery challenges facing training directors, academic programs, and agency leaders who must build scalable domestic violence training systems. The distinction matters because scaling introduces constraints that individual professional development paths do not encounter: instructor capacity, assessment reliability, cost per trainee, and the need to credential cohorts of twenty or fifty clinicians at once rather than one at a time.
The labor market reality compounds the challenge. Therapists with domestic violence specialist certification often earn salaries comparable to generalist mental health counselors, yet the clinical demands include crisis intervention, court testimony, and coordination across law enforcement and child welfare systems. Training programs that ignore these realities produce graduates unprepared for the setting or unwilling to stay in the field.
What Training Do Domestic Violence Therapists Need?
The landscape of domestic violence (DV) therapist training is defined by a combination of state mandates, recommended evidence-based modalities, and the unique demands of working with survivors. Understanding this landscape is essential for clinicians seeking to provide competent, ethical care.
State-Level Training Mandates: A Patchwork of Requirements
Licensing boards set the floor for DV training, but requirements vary dramatically. California mandates 15 hours of DV coursework for license eligibility, one of the more robust state standards. In contrast, Florida requires just 2 hours of domestic violence education every third licensing renewal period. Many states, such as Texas and New York, do not specify a standalone DV training mandate for general mental health licensure, leaving the onus on individual clinicians to seek out specialized education. This wide range, from 2 to 15-plus hours, illustrates the gap between minimal licensure and competent practice.
Beyond state boards, advanced certifications offer a pathway to deeper specialization. For example, the National Advocate Credentialing Program (NACP) sets hour-based tiers for victim advocates, while the Certification for Batterer Intervention Program Facilitators requires extensive training in offender dynamics. Clinicians pursuing trauma-specific certifications often accumulate 40 or more hours of focused DV training.
Core Evidence-Based Modalities for DV Therapists
Several therapeutic approaches are central to DV work, each with defined training milestones:
- Trauma-Focused Cognitive Behavioral Therapy (TF-CBT): A SAMHSA-recognized model for children and adolescents exposed to violence.1 Certification includes 11 hours of web-based training2 plus 16 hours of live, in-person instruction,3 followed by case consultation.
- Cognitive Processing Therapy (CPT): Widely used for PTSD, CPT certification typically requires a two-day foundational workshop (about 13 hours) and subsequent consultation calls focused on DV-specific cases.
- Eye Movement Desensitization and Reprocessing (EMDR): EMDR basic training spans roughly 50 hours, including didactic and supervised practice. Advanced workshops tailor the protocol for complex trauma arising from intimate partner violence.
- Motivational Interviewing (MI): Foundational MI skills are often built through a two-day workshop (around 12-16 hours), with advanced training emphasizing the ambivalence survivors face in safety decision-making.
These hour estimates represent minimal competency building; many clinicians engage in ongoing consultation to reach proficiency in applying each modality with DV populations.
How DV-Specific Training Differs from General Trauma Training
While trauma-informed care is foundational, DV therapy demands additional competencies. Training must address concrete safety planning, including risk assessment using validated lethality instruments. Clinicians learn to recognize coercive control patterns, not just physical incidents, and to understand how these dynamics intersect with child welfare proceedings, custody disputes, and protection orders. This systems-level lens requires not only clinical skill but also working knowledge of legal remedies and community resources. Therapists looking at the full scope of this career path can explore what it means to become a domestic violence counselor before committing to a specialization.
How Many Hours of DV Training Do Therapists Need?
The short answer depends on your state and career goals. For meeting basic licensure requirements, expect anywhere from zero to 15 hours, as noted above. For competent general practice with DV survivors, most experts recommend a minimum of 40 hours of specialized training, blending didactic content with skills practice. Pursuing a full certification in a modality like TF-CBT or EMDR can add another 20-50+ hours. Ultimately, therapists committed to excellence in this field often invest 100 hours or more across multiple trainings and supervised experience.
Therapist Vs. Advocate Vs. Batterer Interventionist: Role Differentiation
What is the difference between a domestic violence therapist, a domestic violence advocate, and a batterer interventionist?
Core Functions and Clientele
Domestic violence therapists focus on mental health treatment. Their typical clients include individuals with trauma-related conditions, such as survivors, offenders, or affected family members. The primary goal is symptom reduction, processing trauma, and improving daily functioning through clinical methods.1
Domestic violence advocates work directly with survivors of intimate partner or sexual violence. Their role centers on safety planning, empowerment, and helping clients navigate systems like housing, legal aid, and protective orders. Advocates do not provide therapy; they offer resources and emotional support to help survivors make informed decisions.1
Batterer interventionists work with individuals who have used violence. Their clients are court-mandated or self-referred perpetrators. The focus is on stopping violent behavior, promoting accountability, and reducing the likelihood of re-assault. Interventionists lead psychoeducational groups aimed at changing attitudes and behaviors, rather than treating underlying mental health disorders.2
Education and Licensure
The educational pathways and credentialing for these roles differ significantly. A domestic violence therapist must hold at least a master's degree in a relevant field such as counseling, social work, or psychology, and is required to obtain a state clinical license to practice independently.2
Advocates often enter the field with a high school diploma or some college. While many have bachelor's degrees, no advanced degree or clinical license is mandated.3 Training is typically provided on the job or through state-certified advocate training programs.
Batterer interventionists follow a separate track. State standards vary, but most require completion of a specialized training program rather than a clinical degree. A mental health license is not always required; however, facilitators must meet state-approved competency standards and often have backgrounds in social services, corrections, or related fields.2
System Integration and Goals
These professions operate within distinct systems. Therapists are integrated into the healthcare system, often working in private practices, hospitals, or community mental health clinics. Their interventions are reimbursable through health insurance.
Advocates function within the domestic violence service system, closely tied to shelters, hotlines, and legal advocacy programs. They also collaborate with law enforcement and courts to support survivors' rights and safety.1
Batterer intervention programs are embedded in the criminal justice and probation systems. Participants are typically mandated by courts, and program completion is monitored by probation officers. The focus is on compliance and behavioral change within a legal framework.2
Why the Distinction Matters for Scalable Training
When building scalable training programs, understanding these role boundaries is essential. Each requires distinct curricula, supervision models, and competency assessments. A one-size-fits-all approach fails to equip professionals with the role-specific skills they need. For instance, advocates need crisis intervention specialist training and systems navigation skills, while therapists require in-depth clinical instruction in evidence-based trauma treatments. Interventionists need training in group facilitation models like the Duluth curriculum. Recognizing these differences ensures that scalable programs remain both efficient and effective.
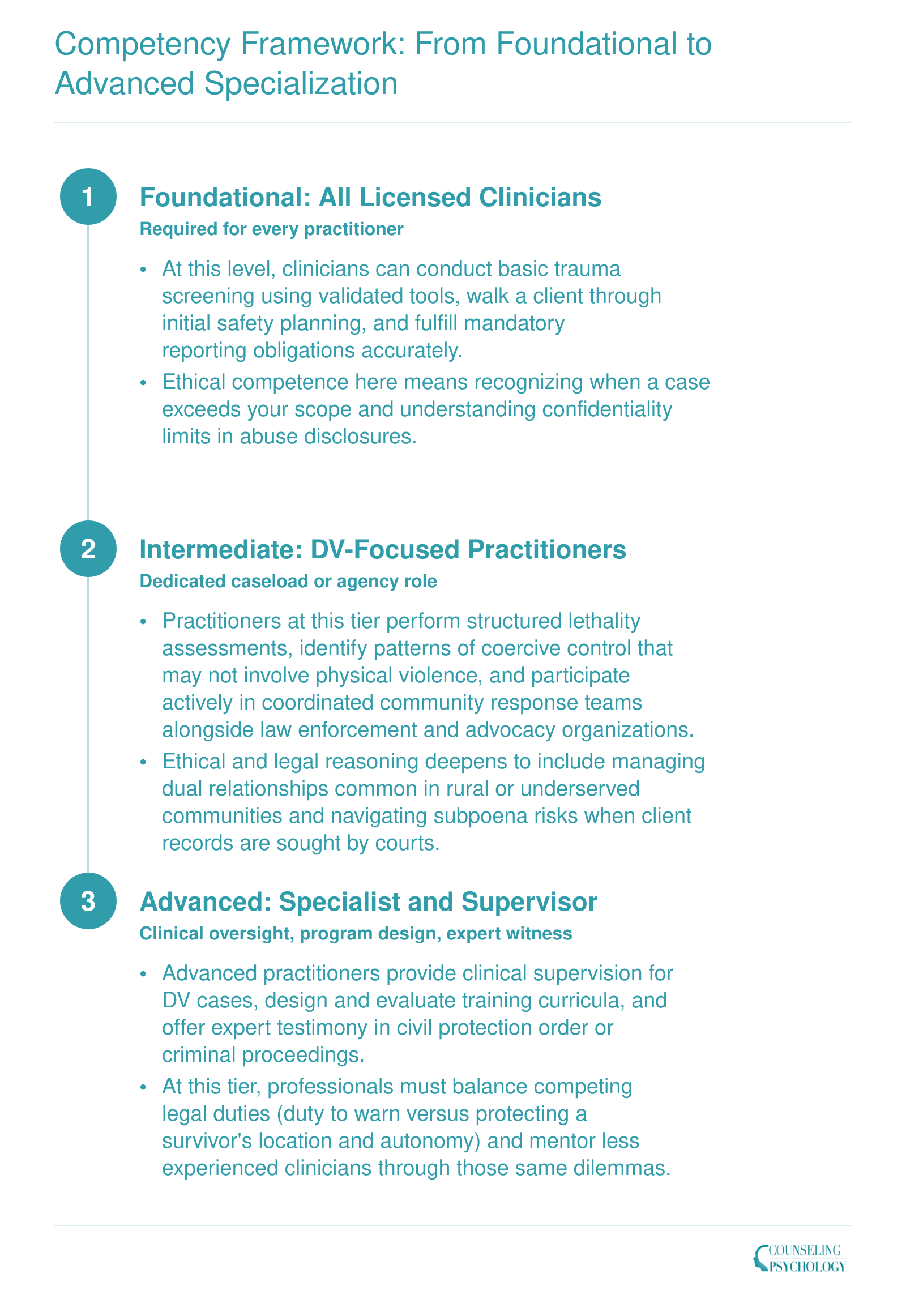
Competency Framework: From Foundational to Advanced Specialization
Not every clinician who encounters domestic violence needs the same depth of training, but every clinician needs some. The three-tier competency model below maps the skill expectations that scale from baseline clinical literacy to specialist-level expertise. Notice how ethical and legal complexities (dual relationships in small communities, subpoena risk, and the tension between duty-to-warn obligations and victim safety) intensify at each stage.
Related Articles
Designing a Scalable Curriculum: Core Components and Delivery Models
One-size synchronous training versus modular self-paced learning: both approaches appear across the domestic violence field right now, and the difference matters enormously when an organization needs to train dozens of clinicians without disrupting caseloads.
What the Current Landscape Looks Like
The training programs operating in 2026 span a wide range of formats. The University of Maine's Intimate Partner Domestic Violence Intervention Training runs as a 12-contact-hour synchronous cohort via Zoom, capped at 45 participants per session.1 That structure suits organizations that want group cohesion and real-time discussion, but it limits throughput. On the other end of the spectrum, the New Jersey Coalition to End Domestic Violence offers a 40-hour web-based program that participants complete at their own pace, removing scheduling barriers for shift workers and rural clinicians.2 Illinois runs a similar self-paced model through its state coalition, requiring 20 hours of online modules for DV professional certification.3
New York's Office for the Prevention of Domestic Violence takes a middle path, offering live virtual sessions on topics like Domestic Violence 101 through a dedicated platform.4 That format preserves some interactivity without requiring everyone to be in the same city.
For shorter professional development needs, the Center for the Application of Substance Abuse Technologies (CASAT) built a 1.5-CEU course on domestic violence and coercive control delivered through the Tovuti platform in both self-paced and live webinar formats.5 The dual-format option means a supervisor can assign the self-paced version to new hires while directing experienced staff toward the live session for discussion-heavy content.
Blended Models and Networked Resources
Blended delivery has emerged as a practical compromise. Anew's 40-hour domestic violence training pairs online modules with in-person components, letting organizations assign foundational content digitally before bringing staff together for skills practice.6 Maryland's behavioral health training approach follows a similar logic, using implementation training videos and downloadable materials that clinical supervisors can deploy asynchronously across multiple sites.7
The Ohio Domestic Violence Network runs an eLearning network that combines online modules, short courses, video content, and embedded quizzes, essentially functioning as a library that agencies can draw from based on staff role and experience level.8 The National Center on Domestic Violence, Trauma and Mental Health maintains an ongoing national webinar series that keeps licensed clinicians current without requiring travel or extended leave.9
Choosing the Right Architecture for Scale
When designing a curriculum meant to reach large numbers of clinicians, program leaders should weigh a few structural questions:
- Cohort size: Synchronous models cap scale; self-paced modules do not, but they require stronger content design to maintain engagement without a facilitator present.
- Credential alignment: Programs tied to state certification requirements, as seen in New Jersey and Illinois, tend to see higher completion rates because participation carries a concrete professional consequence. Clinicians researching the full credential pathway can find role-specific detail in a certified domestic violence counselor guide.
- Role differentiation: A single curriculum rarely serves every staff member equally. Tiered tracks, one for intake staff, one for licensed therapists, and one for supervisors, prevent advanced clinicians from sitting through foundational content they already know.
- Assessment and quality control: Quizzes, case simulations, and post-training competency checks are easier to embed in platform-hosted modules than in live sessions, and they generate data program leaders can use to evaluate effectiveness over time.
For organizations researching what is available before building internally, the training sections of Futures Without Violence and the National Center on Domestic Violence, Trauma and Mental Health are reasonable starting points. State coalition websites, particularly in New York, New Jersey, Illinois, and Ohio, often publish curriculum outlines that can inform local program design without requiring development from scratch.
Questions to Ask Yourself
Certification Paths and Continuing Education Requirements
What certifications do domestic violence therapists actually need, and how do continuing education requirements vary by license type?
The answer depends on three layers: your state's mandates, your specific license category, and whether you pursue a voluntary specialty credential. Sorting through these layers is essential for both individual therapists and program leaders designing scalable training.
Start With Your State Licensing Board
Every state licensing board sets its own rules for LPCs, LCSWs, and LMFTs, and some states require a specific number of domestic violence training hours as part of initial licensure or renewal. Contact your state board directly to confirm what is mandated for your credential. Requirements can shift from one renewal cycle to the next, so checking annually is a sound habit. The Bureau of Labor Statistics (BLS.gov) also maintains links to state-level credentialing resources, which can point you toward the right regulatory body.
National and Specialty Credentials
Beyond state licensure, several organizations offer DV-focused certifications that signal specialized competence to employers and clients:
- NBCC credentials: The National Board for Certified Counselors offers the National Certified Counselor (NCC) as a broad professional credential. While the NCC is not DV-specific, it establishes a recognized baseline. Visit the NBCC website to explore how specialty certifications can layer on top of it.
- NAFC Certified Domestic Violence Counselor (CDVC): Offered by the National Association of Forensic Counselors, this credential is open at both clinical and non-clinical levels. Candidates complete required coursework, pass an oral exam, and submit a letter of intent. The approximate cost is $695.1 Note that CE credit acceptance is not guaranteed across all state boards, so verify before enrolling.1
- YWCA Golden Gate Silicon Valley 75-Hour SA/DV Certification: This 75-hour program covers both sexual assault and domestic violence competencies and costs approximately $425.2 It is open to adults 18 and older who can attend all sessions.
- Casa de la Familia 40-Hour DV Counselor Training: A 40-hour program open to adults regardless of licensure status, useful as foundational training or for advocates transitioning into clinical roles.3
- Eastern Florida State College Domestic Violence Services Certificate: An 18-credit academic certificate costing approximately $1,900.4 CE credit acceptance is conditional, so confirm with your licensing board before counting it toward renewal.
Professional Associations and Continuing Education
Organizations such as the American Association for Marriage and Family Therapy (AAMFT) and the National Association of Social Workers (NASW) maintain continuing education catalogs that frequently include trauma-informed care and domestic violence modules. These can help licensed professional counselors meet renewal requirements while deepening DV-specific skills. Many of these offerings are available online, making them practical building blocks for scalable training programs.
Aligning CE Credits With License Renewal
Not every DV training program automatically generates CE credits that your board will accept. Before investing time or money, confirm three things:
- Whether the training provider is approved by your state's licensing board or by a recognized national accreditor.
- How many DV-specific hours your state requires per renewal cycle, if any.
- Whether the credential you earn will be recognized by employers in your practice setting.
Program leaders building scalable curricula should design modules that meet the most common CE approval standards so graduates can apply their training toward renewal in multiple states. This kind of portability is what separates a niche workshop from a genuinely scalable program.
State-Level Variation in DV Training Mandates
How many hours of domestic violence training do therapists actually need to meet licensure requirements? The answer depends entirely on where they practice. Across the United States, state licensing boards set widely varying standards for domestic violence training, creating a patchwork of requirements that program designers must navigate when building scalable training initiatives.
The Range: From Zero to Voluntary Certification
As of 2026, most states do not mandate specific domestic violence training hours for initial licensure as a therapist. California, New York, Illinois, Washington, Oregon, Texas, and Massachusetts all require zero hours of DV-specific training for LMFTs, LCSWs, LPCCs, LMHCs, or LCPCs at the point of initial licensure.1 However, California does require seven hours of child abuse assessment training and six hours of suicide risk assessment training,1 suggesting that the state prioritizes certain crisis intervention topics over others in its core licensure standards.
Florida represents a different approach: the state requires two hours of domestic violence continuing education for LCSWs, LMHCs, and LMFTs, but only once every six years during the renewal cycle.2 This modest requirement establishes a baseline awareness expectation without imposing a significant burden on practitioners.
For therapists who seek to specialize, California offers a voluntary domestic violence counselor certification pathway that requires 40 hours of specialized training.3 Providers who work with both substance abuse and domestic violence populations can pursue a dual certification requiring 65 to 75 hours of combined coursework.4 These voluntary credentials signal deeper expertise but remain outside the mandatory licensure framework.
Building Modular Curricula Around the Highest Standards
This uneven landscape presents both a challenge and an opportunity for program designers. A scalable training program cannot simply target the lowest common denominator. Instead, effective programs build a modular curriculum anchored to the most rigorous standards, then offer shorter completion tracks for practitioners in states with minimal requirements.
For example, a comprehensive 40-hour core curriculum satisfies California's voluntary certification standard and far exceeds Florida's two-hour renewal requirement. Practitioners in Florida can complete a condensed module drawn from that same curriculum, while California-based therapists pursue the full certification track. This approach ensures consistency in educational quality while accommodating regulatory variation.
Minimum Requirements Are Not Competency Ceilings
Program leaders should remember that state mandates represent minimum floors, not competency ceilings. A therapist who completes only two hours of DV training every six years may meet Florida's legal requirement but will lack the depth needed to effectively serve survivors or manage complex trauma presentations. Scalable programs should aim to exceed the highest state requirement by at least 20 percent, building in advanced topics such as trauma-informed care, cultural responsiveness, and evidence-based interventions that go beyond regulatory checkboxes. supervision hours for counselors and therapists follow a similarly uneven state-by-state pattern, and the design logic for navigating those gaps translates well here.
By designing for the most stringent standards first, training programs create a durable framework that adapts to future regulatory changes and positions graduates to practice competently across state lines.
The median annual wage for mental health counselors and marriage and family therapists hovers around $50,000, yet domestic violence work demands advanced trauma training, crisis readiness, and high emotional labor. This pay-to-intensity gap makes it essential for training programs to equip therapists with self-care strategies and career-sustaining skills, not just clinical competencies, to prevent burnout and turnover.
Salary and Career Outlook for Domestic Violence Therapists
The Bureau of Labor Statistics does not track domestic violence specialization as a separate occupation. Therapists working with DV populations typically fall under one of two broader categories shown below. Because median salaries in these fields are modest relative to the intensity of the work, training program leaders should factor compensation realities into program design. Employer-sponsored training and grant-funded continuing education become essential tools for sustaining a qualified workforce when clinicians cannot easily absorb specialty training costs on their own.
| Occupation | Total National Employment | 25th Percentile Salary | Median Salary | 75th Percentile Salary | Mean Salary | Projected Job Growth (2024 to 2034) | Projected New Jobs |
|---|---|---|---|---|---|---|---|
| Substance Abuse, Behavioral Disorder, and Mental Health Counselors | 440,380 | $47,170 | $59,190 | $76,230 | $65,100 | 17% | 81,000 |
| Marriage and Family Therapists | 65,870 | $48,600 | $63,780 | $85,020 | $72,720 | 13% | N/A |
Adapting Training for Different Practice Settings
A therapist doing 60-minute weekly sessions in a private practice office and a clinician embedded in a 30-day emergency shelter are technically doing the same job, but the clinical demands barely overlap. Scalable training programs have to acknowledge that reality by pairing a shared foundational core with setting-specific electives.
The Five Practice Settings That Shape Clinical Demands
Most domestic violence therapists work in one of five environments, each with its own pressures:
- Emergency shelters: Short treatment windows (often 30 to 90 days), crisis stabilization, safety planning, and group work in congregate living where confidentiality is fragile.
- Private practice: Longer-term trauma processing, insurance and billing navigation, and heavier reliance on evidence-based protocols like CPT, EMDR, or TF-CBT.
- Hospital and emergency department settings: Rapid assessment, lethality screening, mandated reporting decisions in real time, and warm handoffs to community resources.
- Court-based and forensic programs: Documentation that may become evidence, testimony preparation, working with mandated clients, and understanding protective order processes.
- Child protective services partnerships: Pediatric trauma expertise, dyadic parent-child interventions, and navigating dual-client dynamics when a caregiver is both a survivor and a subject of a CPS case.
Core Curriculum Plus Elective Modules
A scalable program teaches every trainee the same foundation: trauma neurobiology, coercive control dynamics, safety planning, cultural humility, and vicarious trauma management. On top of that core, learners select elective tracks matched to their setting. A court-based clinician takes forensic documentation and expert witness preparation. A shelter clinician takes group facilitation and brief-intervention models. A CPS-linked therapist takes attachment-focused pediatric work, drawing on skills common to child welfare social work. This modular structure lets a single training infrastructure serve very different practitioners without diluting either the shared language or the specialized skill.
Cross-Setting Exposure Builds the Coordinated Community Response
Even therapists who plan to spend their entire career in one setting benefit from spending training hours shadowing others. A private practice clinician who has never sat in a shelter intake or observed a protective order hearing will struggle to make effective referrals or interpret what a client means when she says the advocate told her something contradictory. The coordinated community response model only works when each professional understands the others' constraints, timelines, and documentation practices. Build cross-setting rotations or case-conference observations into the training arc, even briefly, and graduates leave with a systems-level fluency that no single-setting curriculum can produce.
Key Considerations for Program Leaders and Educators
Scalable training programs for domestic violence therapists succeed or fail based on the infrastructure decisions program leaders make long before the first cohort enrolls. The curriculum itself is only one piece; assessment, supervision, cultural integration, and funding models determine whether a program can grow without sacrificing quality.
Moving Beyond Written Exams for Competency Assessment
Evaluating a therapist's readiness requires direct observation of clinical skills, not just knowledge recall. Programs designed for scale should incorporate multiple assessment layers:
- Standardized patient encounters: Trainees demonstrate trauma-informed interviewing with trained actors portraying survivors in crisis, assessed using rubrics aligned to your tiered competency framework.
- Supervised case reviews: Audio or video recordings of real sessions are reviewed by faculty using structured rating forms, capturing skills like safety planning and validation.
- Portfolio-based assessment: Learners compile documentation of their work over time: case conceptualizations, treatment plans, and self-reflections, providing a developmental picture of growth.
- Rubric alignment: Each assessment task maps directly to the competency levels defined earlier (foundational, intermediate, advanced), ensuring consistent evaluation standards across cohorts even when multiple raters are involved.
Supervision Models Built for Scale
Traditional one-on-one supervision crumbles when enrollment expands. Adopt a layered approach:
- Group supervision with recorded sessions: Small groups (4-6 trainees) review anonymized recordings together, guided by a senior supervisor. This normalizes feedback and reduces one-on-one time burden.
- Peer consultation structures: Trained peer triads or quads meet weekly to discuss cases, using a structured protocol that keeps conversations focused and productive.
- Tiered supervision: Advanced trainees (those in the specialization phase) co-supervise foundational-level learners under a licensed supervisor's oversight, creating a pipeline of future clinical supervisors and lowering cost-per-trainee.
Embedding Cultural Competency Across the Curriculum
A standalone module on "cultural competence" cannot prepare therapists for the real complexity of domestic violence work. Infuse culturally responsive practice into every unit:
- Immigrant survivors: Teach nuanced safety planning that addresses immigration status threats, language barriers, and distrust of systems.
- LGBTQ+ intimate partner violence: Integrate exercises on power and control dynamics specific to same-sex relationships, bi-erasure, and transgender-specific coercive control.
- Disability-related abuse: Include case examples where perpetrators withhold mobility devices, medications, or communication access.
- Rural access barriers: Practice telehealth adaptations for rural mental health and map local resources when the nearest shelter is 90 miles away.
Building a Sustainable Training Engine
No training program lasts without a realistic funding and partnership strategy:
- Diversify revenue streams: Blend grant funding (federal VOCA, state coalitions) with tuition-based models and employer-sponsored contracts from behavioral health agencies seeking to upskill their workforce.
- Partner with state coalitions: These organizations often maintain training registries and can channel learners toward your program while providing subject matter experts for instruction.
- Track and report outcomes: Collect data on licensure exam pass rates, employment in DV settings, and employer satisfaction. Use these metrics to market the program and secure ongoing funding. A simple dashboard that shows completion rates and post-training job placement can be the most powerful tool in a grant renewal package.
Frequently Asked Questions About DV Therapist Training
These are some of the most common questions we hear from clinicians and program developers exploring domestic violence specialization. Each answer draws on the competency frameworks, certification paths, and curriculum considerations discussed throughout this guide.