What you’ll learn in this article…
- MFTs apply a family systems lens across SAMHSA's three disaster response phases, treating relational damage alongside individual trauma.
- Between 30 and 50 percent of disaster-exposed children develop significant PTSD symptoms, yet most never receive crisis counseling.
- BLS projects 13 percent job growth for MFTs from 2024 to 2034, with disaster behavioral health driving new specialty roles.
- Telehealth now lets deployed MFTs deliver family therapy across state lines, though licensure portability and confidentiality rules vary by jurisdiction.
Why can one family hold together after a hurricane while another collapses under the same stress? In the immediate aftermath of a disaster, couples often report closer bonds: research on Hurricane Harvey survivors found a temporary rise in relationship satisfaction. But that early cohesion frequently masks deeper fractures in communication, parenting, and roles that traditional mental health responders, trained to treat individuals, can miss. Marriage and family therapists (MFTs) bring a relational lens that sees these hidden breakdowns.
Disaster behavioral health frameworks are now formally recognizing that family-systems approaches improve recovery outcomes. SAMHSA's guidelines increasingly call for therapists addressing the interplay between individual trauma and family functioning. MFTs trained in disaster competencies, telehealth, and crisis ethics are stepping in as core responders to the family wounds that raw hardship leaves behind.
What Makes MFTs Uniquely Suited for Disaster Response
When communities are shattered by disaster, the immediate mental health response often prioritizes individual trauma symptoms, but the hidden casualties are the family systems that fall apart silently. Marriage and family therapists (MFTs) bring a relational lens that separates them from other mental health professionals, directly targeting the family unit's ability to recover and reorganize after catastrophic events.
A Systems Lens That Individual-Focused Approaches Miss
Most mental health clinicians are trained to treat one person at a time. Psychologists typically approach disaster survivors through assessment and diagnosis of acute stress or PTSD, while licensed professional counselors (LPCs) and clinical social workers (LCSWs) often center on individual coping strategies and emotional regulation. MFTs are different: their entire clinical education is built on systems theory, which holds that a person's distress cannot be fully understood or treated outside of their key relationships. For those curious about the training pathway, our guide on how to become a marriage and family therapist outlines the educational and licensure steps involved. In a disaster context, this means MFTs look past the presenting symptoms of anxiety or withdrawal and ask how the crisis has disrupted communication patterns, altered family roles, and strained the caregiving network.
Disasters do not wound in isolation. A hurricane, wildfire, or mass violence event can erase a home, scatter extended family, force adult children into caretaking roles for traumatized parents, and turn spouses into exhausted survival partners who no longer connect emotionally. These role reversals, communication breakdowns, and caregiver strains are systemic ruptures that demand a systemic intervention. MFTs are deliberately trained to work with the couple or family as the client unit, making them uniquely prepared to address the relational damage that unfolds after a disaster.
Structural and Strategic Therapy Models Map Directly onto Disaster Recovery
MFT programs place heavy emphasis on classical family therapy models that are remarkably well suited to post-disaster realities. Structural family therapy, for example, focuses on reorganizing family boundaries and hierarchies, exactly the kind of restructuring needed when a family's previous routines, rules, and roles have been upended by an emergency. Strategic family therapy brings problem-focused, directive techniques that help families develop concrete solutions to new practical and relational challenges, such as sharing caregiving duties for displaced elders or managing conflict over scarce resources. These models give MFTs a ready toolkit for guiding families from chaos toward a functional new normal, not merely helping each member cope alone.
Why This Distinction Matters in Emergency Response Planning
Without an MFT's systemic perspective, disaster behavioral health responses can miss the core unit that will carry survivors through long-term recovery. When family systems remain fractured, individual symptoms persist or return, even after individual counseling. MFTs fill a documented gap in traditional disaster mental health teams, where the primary focus is triage and immediate psychological first aid. Beyond disaster work, MFT-trained professionals can apply their systems expertise across a range of settings; our overview of MFT career paths explores several of these options. By incorporating family-systems expertise early, response planners strengthen the entire relational infrastructure that communities depend on to heal. MFTs are not just another clinician on the roster but a distinct, essential resource for disaster-affected families.
Phases of Disaster Response and MFT Interventions
The Substance Abuse and Mental Health Services Administration (SAMHSA) identifies three phases of disaster behavioral health response: immediate, intermediate, and long-term. Marriage and family therapists (MFTs) adapt their interventions to each phase, applying a family systems lens to support recovery and resilience.
Immediate Phase (0, 4 Weeks): Stabilizing Families
The immediate aftermath demands rapid, practical support. MFTs provide Psychological First Aid (PFA) adapted for families, focusing on safety, emotional connection, and access to basic needs. When family members are separated (common during evacuations), therapists help with reunification by coordinating with shelters and emergency services. Crisis communication work centers on normalizing stress reactions and preventing blame or escalation. Screenings identify family-level risk factors such as pre-existing conflict, domestic abuse survivor counseling needs, or a caregiver's mental health condition, which predict poor recovery. MFTs collaborate with first responders to ensure that family units, not just individuals, receive stabilizing care.
Intermediate Phase (1, 6 Months): Rebuilding Relationships
As immediate shock subsides, relationship strain emerges. Couples may argue over financial stress or changed roles; children act out as routines dissolve. MFTs guide families in grief counseling, naming losses of home, community, or a loved one within a safe relational container. They assist in rebuilding daily roles and routines, restoring a sense of predictability. Critically, they identify children's needs by observing behavioral regression, academic struggles, or withdrawal, and help parents respond without adding pressure. Family sessions in this window often focus on renegotiating responsibilities and validating each member's experience.
Long-Term Recovery (6+ Months): Healing as a Family System
Lasting mental health impacts surface when external aid fades. MFTs treat PTSD and depression through a relational lens, recognizing that individual symptoms ripple through the family. They facilitate collective trauma narrative work: families construct a shared story of survival and meaning, which buffers against intergenerational transmission. Domestic violence often escalates under chronic stress; MFTs screen routinely and connect survivors to legal and shelter resources. For multigenerational households, therapy acknowledges cultural strengths and strains, supporting elders and children simultaneously. This phase ends not with a return to pre-disaster life, but with the family's newly integrated identity.
The 4 C's of Disaster Recovery Through a Family Lens
MFTs operationalize communication, collaboration, community, and commitment in every phase:
- Communication: Families learn to express needs without blame, listen actively, and resolve conflicts that trauma amplifies.
- Collaboration: Therapists coordinate with schools, medical providers, and disaster agencies to create a wraparound support system.
- Community: MFTs build and facilitate support groups that reconnect families with neighbors and cultural traditions.
- Commitment: Long-term follow-up and booster sessions prevent relapse and honor the nonlinear nature of healing.
How Disasters Affect Marriages, Couples, and Family Relationships
The immediate aftermath of a natural disaster can sometimes pull couples closer together. Research on marriages affected by Hurricane Harvey found an initial surge in relationship satisfaction, especially among couples who were least satisfied before the storm struck.1 Yet that boost proved temporary: satisfaction returned to baseline within about 12 months, and the severity of material losses did not significantly predict stronger bonding.1 Meanwhile, other indicators paint a more troubling picture. During the COVID-19 pandemic, international studies documented a 20 to 30 percent rise in calls to domestic violence hotlines, signaling escalated conflict behind closed doors.2 Divorce rates often dip immediately after a disaster, partly because of practical barriers like court closures, but the underlying relational strain can fester. Mexico saw a 43 percent decline in divorce filings early in the pandemic, with filings recovering within six months.2 These patterns suggest that while some families rally together, many experience heightened tension that requires professional support.
Relationship Strain in the Wake of Disaster
Disasters create a cascade of stressors that can overwhelm even resilient couples. Financial hardship is often the most immediate trigger: lost wages, property damage, and insurance battles strain household budgets and provoke blame. Displacement compounds the pressure. Families crammed into temporary housing or relatives' homes lose daily routines, privacy, and the sense of normalcy that buffers conflict. Role confusion surfaces when a primary earner is out of work or a stay-at-home parent suddenly shoulders new financial responsibilities. Parenting challenges escalate as children react to trauma with behavioral regression (bedwetting, tantrums, or clinginess), which exhausts already depleted parents and fuels arguments about discipline and care.
Family Dynamics Under Pressure
Marriage and family therapists (MFTs) observe that disasters amplify pre-existing relationship vulnerabilities. A couple that communicated poorly before a hurricane will find that pattern intensified when stress peaks. Sibling rivalries resurface; parents may favor one child's needs over another's. In severe cases, intimate partner violence spikes. National hotline data consistently shows surges following large-scale disasters, a stark reminder that safety planning within therapy is critical. MFTs are trained to assess for abuse and coordinate with shelters and legal advocates while preserving the therapeutic alliance where it is safe to do so. Professionals who specialize in childhood trauma counseling often collaborate with MFTs during these interventions to address the needs of younger family members.
Multigenerational and Cultural Stressors
Many households include elderly relatives, and disasters can shift caregiving burdens abruptly. Adult children may become primary caregivers while also managing their own trauma, leading to resentment and exhaustion. Cultural norms shape how families cope: some communities emphasize stoicism or collective problem-solving, while others may mistrust formal mental health support. MFTs bring a systemic lens that honors these dynamics, helping families navigate role changes and cultural expectations without pathologizing their values.
How MFTs Help Couples and Families Recover
A core MFT technique is reflecting feelings, a careful process where the therapist encourages each member to voice their emotional experience and then paraphrases it back, allowing others to hear the speaker's perspective without judgment. In a disaster context, one partner might say, "I feel abandoned when you focus only on the insurance paperwork." The therapist reflects, "So the focus on paperwork leaves you feeling alone and unseen." This simple intervention often defuses blame and opens space for empathy.
Practical interventions tailored to disaster recovery include: - Structured communication exercises: Families practice "I" statements and scheduled check-ins to contain conflict and rebuild trust. - Co-parenting realignment: When displacement separates parents from children, MFTs help renegotiate roles, maintain consistent bedtime routines across households, and preserve secure attachments. The divorce and co-parenting resource section of this site offers additional guidance on navigating these transitions. - Genogram-based trauma mapping: Using a visual family tree, the therapist maps past traumas (such as previous floods or losses) and explores how these shape current reactions, helping the family break maladaptive patterns.
Disasters test relationships, but with the right support, families can emerge with deeper understanding and more adaptive ways of coping.
Related Articles
Questions to Ask Yourself
MFT Disaster Competencies and Training Pathways
Building the skills to serve families in crisis requires deliberate preparation long before a disaster strikes. Fortunately, several well-established organizations offer training specifically designed for mental health professionals who want to work in disaster behavioral health settings.
AAMFT Professional Development Resources
The American Association for Marriage and Family Therapy periodically offers webinars, online courses, and continuing education units focused on trauma, crisis intervention, and disaster mental health. Offerings change throughout the year, so checking the AAMFT website directly under its professional development section is the most reliable way to find current schedules. Some offerings are free to members, making active membership a practical advantage for MFTs who want affordable continuing education in this area.
American Red Cross Mental Health Volunteer Pathways
The American Red Cross deploys licensed mental health professionals during disaster relief operations, and MFTs can qualify for this work in many states. Eligibility requirements, credentialing standards, and available volunteer roles vary by region and are subject to change. Visiting redcross.org or contacting your local chapter directly will give you the most accurate picture of what is currently required and how to begin the application process. Once accepted, volunteers typically complete Red Cross-specific training before being deployed to a shelter or disaster site. MFTs interested in complementary specializations, such as crisis counselor training, may find those credentials strengthen their applications.
FEMA Crisis Counseling Program Roles
FEMA's Crisis Counseling Program, administered through SAMHSA, funds state-level mental health services after presidentially declared disasters. MFTs can play meaningful roles within CCP-funded projects, though hiring and eligibility are managed at the state level through emergency management agencies and designated mental health authorities. SAMHSA's CCP page is a useful starting point for understanding how the program works nationally, while your state's emergency management agency can clarify current openings or partnership opportunities.
Certifications and Graduate Programs
The National Board for Certified Counselors offers a disaster mental health specialty credential. Requirements, application windows, and fees are detailed on nbcc.org and should be verified directly, as credentialing standards evolve. For MFTs who want more structured academic preparation, some universities with COAMFTE-accredited programs offer marriage and family therapy certificates in disaster behavioral health or trauma-focused care. These certificates can often be completed alongside or after a master's degree. When researching programs, confirm accreditation status, whether coursework can be completed online, and how the curriculum addresses the family systems lens that distinguishes MFT practice from other mental health disciplines.
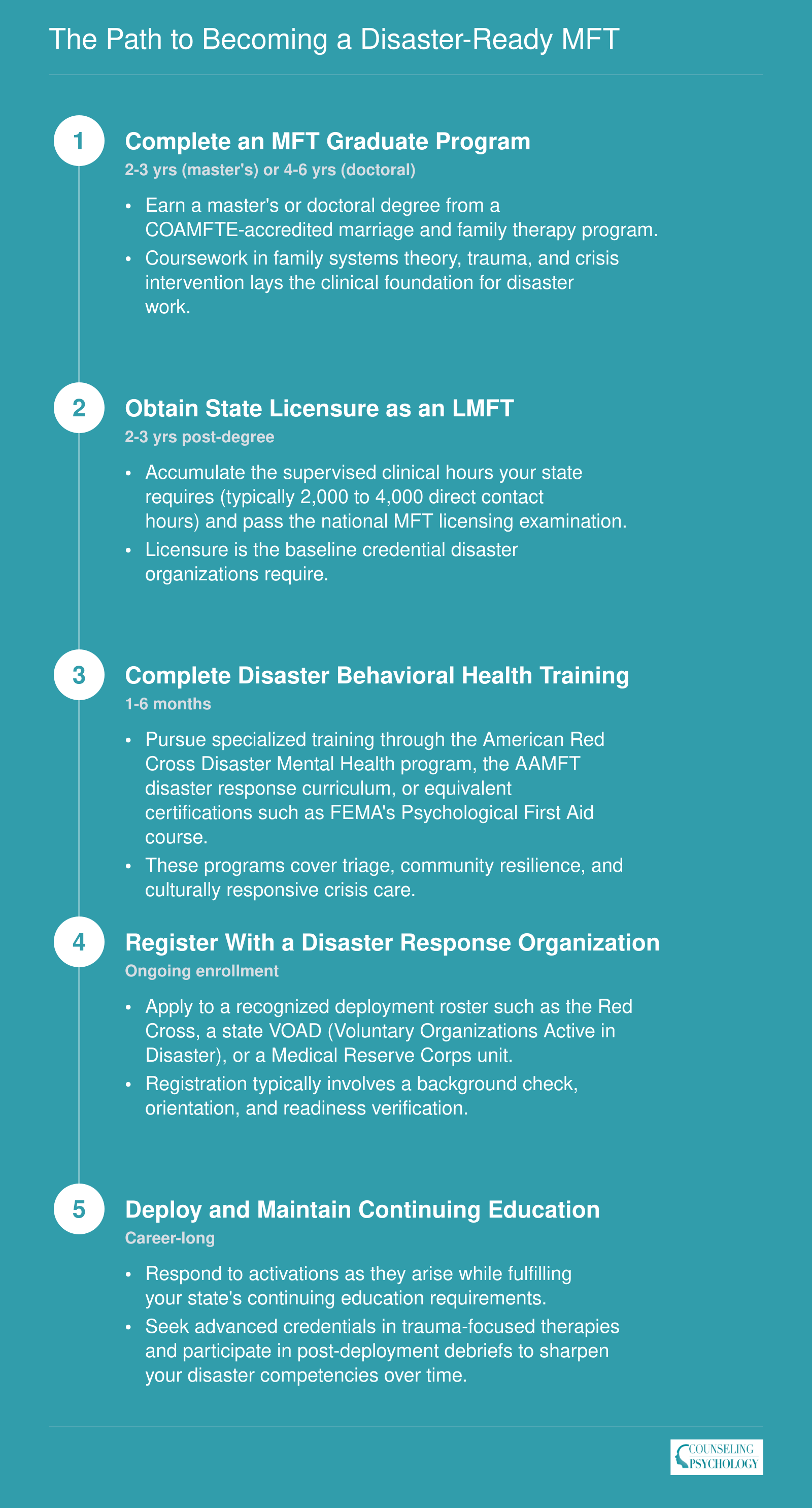
The Path to Becoming a Disaster-Ready MFT
Moving from graduate student to deployed disaster therapist follows a clear credentialing sequence. Each step builds on the last, so planning ahead can shave months off the timeline.
Telehealth and Technology in Disaster Family Therapy
In-person sessions in a clinic versus remote sessions from a shelter cot or a relative's spare bedroom: that is the reality MFTs face when disasters displace entire families across counties or state lines. Telehealth has shifted from a convenience to a necessity in post-disaster family therapy, yet the regulatory and practical landscape for marriage and family therapists remains more restrictive than many practitioners realize.
Why Telehealth Becomes the Default After a Disaster
When flooding, wildfires, or hurricanes destroy local infrastructure, traditional office-based therapy is often impossible. Families scatter to temporary housing, shelters, or the homes of distant relatives. Children may be enrolled in schools hours away from parents who stayed behind to manage insurance claims. In these situations, gathering every family member in the same room for a structural or strategic family therapy session is simply not feasible. Telehealth platforms that support multi-participant video calls allow therapists to reconvene a displaced family system, even when members are spread across multiple states. For clinicians exploring this modality full-time, understanding the steps to become a licensed telehealth therapist is an important foundation.
The Regulatory Gap Facing MFTs
As of 2026, MFTs do not have an operational interstate practice compact.1 Psychologists benefit from PSYPACT, which now covers 40-plus states.2 Licensed professional counselors can use the Counseling Compact, which is active and issuing credentials.3 Even social workers have an enacted compact in at least seven states, though it has not yet begun issuing licenses.4 MFTs, however, lack model compact legislation entirely.5 That means the default rule still applies: an MFT must hold a full, active license in every state where a client is physically located during a session.6
During a federally or state-declared disaster, governors can activate emergency licensure waivers that temporarily allow out-of-state clinicians to practice. These waivers typically last 30 to 180 days and often require the therapist to register with the disaster state's licensing board and, in some cases, practice under supervision.7 The window is helpful but narrow, and MFTs who want to continue treating displaced families beyond that period must pursue full licensure or hold dual licenses in advance.
Practical Considerations for Remote Family Sessions
Running a family therapy session over video introduces challenges that go beyond a stable internet connection:
- Platform requirements: Multi-person sessions need a HIPAA-compliant platform that supports gallery view so the therapist can observe nonverbal cues across participants simultaneously. Standard two-person telehealth setups often fall short.
- Confidentiality in shared spaces: A parent calling from a crowded shelter or a teenager logging in from a grandparent's living room cannot speak freely. Therapists need to assess each participant's environment at the start of every session and may need to schedule brief individual check-ins before bringing the full family together.
- Adapting techniques for video: Structural family therapy interventions like enactments, boundary-making, and seating rearrangements lose their spatial dimension on screen. Clinicians often compensate by using deliberate turn-taking protocols, muting and unmuting strategically to shift alliances, and assigning between-session tasks that recreate relational experiments in the home environment.
What the Evidence Shows (and Where It Falls Short)
Honestly, the outcome data on telehealth-delivered family therapy during disasters is thin. Most published literature focuses on individual trauma treatment or general telehealth satisfaction surveys rather than family systems outcomes in disaster-specific contexts. A handful of case reports from post-hurricane and post-wildfire settings suggest that families who received remote therapy reported improved communication and lower conflict, but these are small-scale observations, not controlled studies. The evidence gap is real, and the field would benefit enormously from systematic research comparing in-person and remote family therapy outcomes in disaster recovery populations.
For MFTs committed to disaster work, staying current on interstate compact developments is not optional. The regulatory landscape is evolving quickly across allied professions, and advocacy for an MFT-specific compact continues within the field. In the meantime, clinicians should identify states where they are most likely to serve displaced families and begin the licensure process proactively rather than relying solely on temporary emergency waivers.
Ethical and Legal Considerations for Deployed MFTs
Ethical and legal considerations for deployed MFTs involve navigating professional boundaries, confidentiality constraints, licensure requirements, and mandatory reporting obligations in settings where standard practice assumptions often do not apply. Disaster work compresses timelines and collapses the usual separations between therapist and community, making proactive ethical planning essential before deployment.
Dual Relationships in Disaster Settings
In small-town disasters or tight-knit communities, an MFT may be a fellow survivor, neighbor, or acquaintance of the families seeking help. These dual relationships are sometimes unavoidable rather than unethical, but they require careful management. Before sessions begin, therapists should acknowledge shared circumstances openly, clarify role boundaries, and document the reasoning for proceeding. When the overlap is too significant (for example, treating a close friend's family), referral to another provider protects everyone involved. Supervision or peer consultation, even by phone, helps MFTs stay accountable when isolation makes objectivity harder to maintain. Therapists still accumulating clinical hours should confirm with their board how disaster-context sessions count toward LMFT supervision hours.
Confidentiality in Congregate Settings
Shelters, community centers, and temporary housing rarely offer private rooms for family sessions. Conducting multi-person therapy when others can overhear requires adaptation:
- Environmental adjustments: Position seating away from high-traffic areas, use white noise apps or portable fans, and schedule sessions during quieter periods.
- Informed consent: Explain the limitations of confidentiality before sessions begin so families can decide what to disclose.
- Documentation: Note the setting constraints in session records to protect both the family and the clinician.
These workarounds do not replace true privacy, but they reduce risk and demonstrate professional diligence.
Cross-State Licensure and Liability
MFTs who deploy outside their home state must verify their legal authority to practice. Many states issue emergency practice waivers during declared disasters, but coverage varies in duration, scope, and documentation requirements. The Psychology Interjurisdictional Compact does not yet include MFTs, so therapists should contact the licensing board in the affected state before providing services. Liability insurance policies differ on out-of-state coverage; confirming that malpractice protection extends to the deployment location prevents gaps that could expose therapists to personal risk.
Mandatory Reporting Obligations
Child abuse, elder abuse, and intimate partner violence reporting requirements remain in effect during disasters. Stress and displacement often increase disclosures during family sessions, placing MFTs in situations where they must act quickly. Clinicians working with cases involving partner violence may benefit from specialized training such as a certified domestic violence counselor credential. Knowing the local reporting hotlines, child protective services contacts, and law enforcement procedures in the disaster zone is as important as clinical preparation. Therapists should brief families early in treatment that certain disclosures will trigger mandatory reports, a step that maintains trust even when the conversation is difficult.
MFT Salary and Career Outlook in Disaster Behavioral Health
Marriage and family therapists occupy a growing niche in disaster behavioral health, and the broader occupational outlook reflects strong demand. According to the Bureau of Labor Statistics Occupational Outlook Handbook, MFTs are projected to see 13% job growth from 2024 to 2034, a rate classified as much faster than average, with roughly 7,700 openings anticipated each year nationally. The national salary data below covers all MFTs regardless of specialty. Disaster behavioral health roles may offer supplemental pay through federal contracts, FEMA crisis counseling programs, or SAMHSA funded initiatives, though dedicated salary data for disaster focused MFT positions is not separately tracked by BLS at this time.
| Metric | National Data for Marriage and Family Therapists |
|---|---|
| Total Employment | 65,870 |
| 25th Percentile Annual Wage | $48,600 |
| Median Annual Wage | $63,780 |
| Mean Annual Wage | $72,720 |
| 75th Percentile Annual Wage | $85,020 |
| Projected Job Growth (2024 to 2034) | 13% (much faster than average) |
| Estimated Annual Openings (2024 to 2034) | 7,700 |
Research compiled by SAMHSA suggests that between 30 and 50 percent of children exposed to disasters develop significant PTSD symptoms, yet after Hurricane Katrina only about 30 percent of survivors in the hardest hit areas received any crisis counseling. That gap highlights an enormous unmet need for family focused clinicians like MFTs in declared disaster zones.
Self-Care and Preventing Compassion Fatigue for MFTs in Disaster Work
Marriage and family therapists who respond to disasters absorb the emotional turmoil of entire family systems, not just individual clients. Watching a couple struggle to co-parent amid displacement or a child regress after witnessing destruction compounds the clinician's emotional load. This systemic immersion, often combined with the therapist's own ties to the affected community, creates a dual-survivor dynamic that heightens vulnerability to compassion fatigue. Extended deployments, limited resources, and the relentless pace of field work can erode empathy and lead to burnout faster than in many other clinical settings.
Why Systemic Work Intensifies Compassion Fatigue
MFTs are trained to hold multiple perspectives simultaneously: the parent's fear, the adolescent's withdrawal, the marital conflict that escalates under stress. In disaster contexts, this multilayered attunement becomes a liability when clinicians lack adequate support. The therapist's own grief over lost homes or disrupted routines may remain unprocessed because the work demands constant outward focus. Without intervention, the cumulative weight of these absorbed narratives can lead to emotional exhaustion, depersonalization, and a sense of reduced professional efficacy.
Organizational Safeguards: Peer Support and Rotations
Agencies and response teams hold the primary responsibility for structural protections. Evidence points to peer consultation structures as a frontline defense: regular, facilitated group debriefings where MFTs share cases and reactions normalize distress and reduce isolation. Deployment rotation schedules that limit continuous field work to two to three weeks, followed by required rest periods, prevent the depletion that comes from prolonged exposure. Supervision models adapted for austere settings, such as daily check-ins with an off-site clinical supervisor via telehealth, offer real-time guidance and emotional containment. These practices must be codified in agency policy, not left to individual goodwill.
Individual Strategies for Austere Environments
Therapists can complement systemic supports with portable, low-tech practices. Brief grounding exercises, such as the 5-4-3-2-1 sensory technique, take under a minute and require no equipment. Diaphragmatic breathing and progressive muscle relaxation can be done in a vehicle between family visits. Even in chaotic settings, a morning ritual of quiet reflection or a brief journal entry helps maintain a sense of personal continuity. The key is selecting methods that are feasible under field conditions; elaborate self-care plans often collapse when exhaustion sets in.
The False Choice Between Self-Care and System Support
Framing resilience as solely a personal responsibility ignores the power dynamics of disaster work. An MFT who practices mindfulness but faces incessant caseloads without managerial backup will still burn out. Conversely, the most well-intentioned organizational policies fail if clinicians ignore their own warning signs. Sustainable practice requires both: leaders who enforce manageable schedules and fund confidential peer support, and therapists who actively use those resources and cultivate internal coping skills. Professionals interested in the broader landscape of acute behavioral health work may also explore the path to becoming a crisis intervention specialist. Neither dimension alone is sufficient.
From Heroic Deployment to Sustainable Practice
Disaster behavioral health should be viewed as a career-long competency, not a singular act of sacrifice. MFTs who commit to ongoing training in disaster competencies, engage in periodic self-assessments, and intentionally pace their involvement build careers that can weather multiple responses. Treating deployment as a marathon rather than a sprint protects not only the clinician but the families they serve. The goal is not to survive one catastrophe, but to remain effective across a lifetime of service.
Frequently Asked Questions About MFTs in Disaster Response
Disaster behavioral health is a growing area of practice for marriage and family therapists. Below are answers to the questions we hear most often from students and early-career clinicians exploring this specialty.