What you’ll learn in this article…
- A 2026 trial of 6,205 college students found digital guided self-help CBT outperformed traditional referral.
- Guided formats cut dropout rates roughly in half compared to unguided programs.
- Digital self-help costs up to 80 percent less per patient than traditional therapy.
More than half of adults who meet diagnostic criteria for a common mental health condition receive no treatment in a given year. Waitlists stretch for months, provider shortages persist in rural and underserved areas, and many individuals who do seek care drop out before completing a meaningful course of treatment. Evidence-based digital self-help programs, structured CBT-based interventions delivered through platforms rather than clinicians, are stepping into that gap.
This is not about wellness apps or general mindfulness tools. The programs examined here are protocol-driven, empirically tested, and in several cases demonstrate effect sizes comparable to face-to-face therapy. A landmark 2026 study led by Michelle Newman of Penn State screened over 39,000 college students and found that a digital guided self-help CBT platform outperformed traditional therapy referral at every follow-up point across two years.1 For practitioners in clinical, counseling, forensic, and social work settings, the relevant question in 2026 is no longer whether these tools work. It is how to evaluate, recommend, and integrate them responsibly.
What Is Digital Self-Help Therapy and How Does It Differ From Digital Therapeutics?
Digital self-help therapy sits on a continuum between fully automated wellness apps and traditional clinician-delivered care, but it is often confused with adjacent categories that serve distinct purposes. Understanding these boundaries helps clinicians choose the right tool for the right patient at the right time.
Defining Digital Self-Help Therapy
Digital self-help therapy refers to app-based or web-based programs that guide users through structured therapeutic content, either independently or with light coaching support. Users work at their own pace, typically moving through modules that teach skills such as cognitive restructuring, behavioral activation, or exposure techniques. These programs are designed to address specific mental health concerns like anxiety, depression, or insomnia, and they rely on evidence-based protocols rather than general wellness advice.
This category differs from three adjacent forms of digital care. Digital therapeutics are FDA-cleared medical devices that must be prescribed by a clinician and meet rigorous regulatory standards. Teletherapy involves live, synchronous sessions with a licensed clinician delivered over video or phone, replicating traditional therapy via remote technology. General wellness apps offer meditation, mood tracking, or journaling features but do not claim to treat clinical conditions and typically lack a peer-reviewed evidence base.
Guided vs. Unguided: The Most Important Distinction
Within digital self-help, the guided versus unguided distinction is the single strongest predictor of outcomes. Guided programs pair the user with a human supporter, such as a trained coach, peer counselor, or clinician, who provides encouragement, answers questions, and monitors progress through asynchronous messages or brief check-ins. Unguided programs are fully self-directed, with no human contact beyond automated prompts or chatbot interactions. Research consistently shows that guided self-help produces larger effect sizes and lower dropout rates than unguided versions, particularly for users with moderate symptom severity.
Therapeutic Foundations and Stepped-Care Context
Most evidence-based digital self-help platforms draw from cognitive behavioral therapy, reflecting CBT's modular structure and strong fit for digital delivery. Emerging programs now incorporate acceptance and commitment therapy, behavioral activation for depression, and exposure-based protocols for anxiety and trauma-related conditions. Digital self-help occupies a middle tier on the intensity continuum: more structured and interactive than bibliotherapy or psychoeducation, but less intensive than weekly therapy sessions. This positioning makes it a natural stepped-care tool, and the mental health workforce shortage has only accelerated demand for it, allowing clinicians to reserve face-to-face slots for complex presentations while extending evidence-based support to patients on waitlists, in maintenance phases, or seeking lower-cost options. It is not a replacement for traditional therapy when clinical complexity, risk, or comorbidity demands direct clinician oversight.
The Evidence Base: How Effective Is Digital Self-Help Across Conditions?
Digital self-help interventions produce measurable symptom reductions across a range of mental health conditions, with effect sizes comparable to face-to-face therapy in many studies. Clinicians evaluating these tools should consult the latest meta-analytic evidence, which demonstrates both the promise and the boundaries of digital delivery.
Depression and Anxiety: Robust Findings Across Multiple Reviews
Digital cognitive-behavioral therapy (CBT) for depression and anxiety disorders has accumulated the strongest evidence base. Meta-analyses published between 2022 and 2024 show moderate to large effect sizes when digital self-help is compared to waitlist controls. For generalized anxiety disorder, one 2022 review reported a pooled Hedges' g of 0.79, indicating a clinically meaningful reduction in symptoms.1 Social anxiety disorder showed an identical effect size (g = 0.79) in the same analysis, while panic disorder demonstrated an even larger benefit (g = -0.89) across 470 participants.1 Obsessive-compulsive disorder interventions also reached g = 0.78, suggesting that anxiety disorders as a category respond well to structured digital protocols.1
For practitioners seeking these findings, the most direct path is searching academic databases such as PubMed, PsycINFO, or Google Scholar with terms like "meta-analysis digital CBT effect size depression anxiety" and filtering results to publications from 2023 through 2026. The Results section or forest plots within meta-analyses will list pooled effect sizes (Cohen's d or Hedges' g), while participant flow diagrams and tables report sample sizes.
Insomnia, Eating Disorders, and Specialty Applications
Digital CBT for insomnia (CBT-I) has shown particularly strong results in workplace populations, with one recent randomized controlled trial for workplace CBT-I reporting a Cohen's d of 1.75 for sleep-quality improvements.3 This outsizes many pharmacological interventions and underscores the viability of self-help for behavior-change targets.
Eating disorders present a more nuanced picture. A 2024 meta-analysis found smaller effect sizes: Hedges' g = 0.24 for at-risk or symptomatic adults, rising to g = 0.39 for individuals meeting clinical diagnostic criteria.2 While these effects are modest, they still represent meaningful harm reduction in a population where access to specialized care is often limited.
College and Workplace Populations: Real-World Uptake Data
A 2026 study of over 6,200 college students across 26 campuses demonstrated that digital guided self-help reduced mental disorder prevalence by 4.3 percentage points more than traditional referral pathways at two-year follow-up.4 This finding underscores not just efficacy under controlled conditions but real-world effectiveness when digital tools are embedded in service delivery systems. Practitioners working with campus counseling centers or rural mental health provider shortages will find this evidence particularly relevant, since digital platforms can extend reach where in-person staffing is thin.
Finding Current Evidence Efficiently
For time-constrained clinicians, authoritative aggregators offer curated access to meta-analyses. The American Psychological Association, the National Institute of Mental Health, and the International Society for Research on Internet Interventions maintain updated repositories and clinical summaries. Umbrella reviews and meta-reviews, which synthesize multiple meta-analyses across conditions, provide pooled effect sizes and are searchable with terms like "umbrella review digital mental health interventions."
Program-level effectiveness data continue to evolve. While early adopters saw variable results, recent trials with improved engagement strategies and coaching support show convergence toward face-to-face benchmarks for mild to moderate presentations.
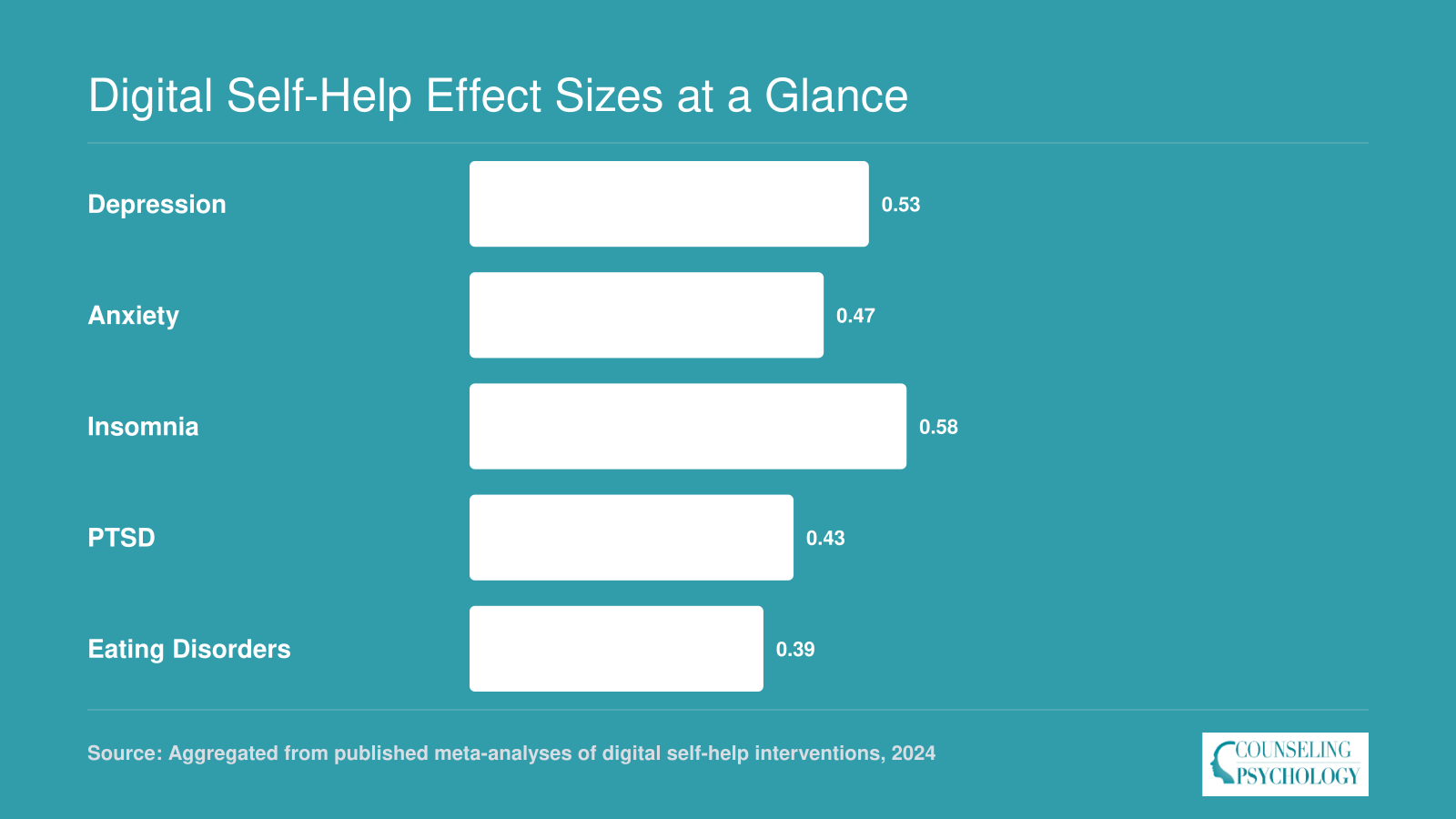
Digital Self-Help Effect Sizes at a Glance
Pooled effect sizes from multiple meta-analyses show that digital self-help interventions produce small to moderate improvements across several common mental health conditions when compared to waitlist controls. These are aggregated estimates; individual study quality, intervention format, and population characteristics vary considerably across the underlying research.
New Research: Digital Guided Self-Help CBT Outperforms Traditional Referral in College Students
A population-based pragmatic randomized clinical trial screened over 39,000 students from 26 U.S. colleges and randomized 6,205 who met criteria for a mental disorder to either a traditional therapy referral or a digital cognitive-behavioral guided self-help (D-CBTgsh) platform.1 The study, led by Michelle G. Newman of Penn State and published in Nature Human Behaviour (Newman et al., 2026; doi:10.1038/s41562-026-02460-1), provides the strongest evidence to date that coached digital interventions can outperform standard referral pathways in real-world campus settings.2
Study Design and Intervention Details
The D-CBTgsh platform targeted three conditions: anxiety, depression, and eating disorders. Participants received 6-8 interactive modules lasting approximately 20 minutes each, delivering core CBT skills.1 Coaches held at least a bachelor's degree, were enrolled in postgraduate mental health training, and attended weekly supervision sessions with a licensed psychologist. This supervision layer ensured fidelity and provided a meaningful safety net, a critical feature for clinicians weighing adoption.
Uptake and Clinical Outcomes
Service uptake alone told a striking story: 74.4% of students assigned to the digital platform engaged with the intervention, compared to just 30.2% who used traditional therapy after referral.3 The headline finding was efficacy: at 6 weeks, 6 months, and 2 years, the digital group showed significantly lower prevalence of any mental disorder. As reported in a July 2026 Psychology Today summary, the therapeutic effects were "superior across the board," sustained even two years later.technology in counseling and psychotherapy is increasingly central to understanding why these outcomes hold over time.
Why This Matters for Clinicians
These results are not a plea to replace human therapy. They are a mandate to rethink default referral pathways. The study demonstrates that a coached digital self-help model can function as an effective stepped-care entry point, reserving scarce counselor time for higher-acuity cases while actively improving outcomes for a broad population. The fact that the digital arm outperformed referral at every follow-up suggests that simply handing students a list of campus resources leaves measurable clinical benefit unrealized. For the practicing clinician, this study offers a clear blueprint: when supported by trained coaches and structured CBT content, digital tools can extend reach without diluting quality, and in many cases, do better than business as usual.
Guided Vs. Unguided Self-Help: When Does Clinician Support Matter?
The question of whether human support improves digital self-help outcomes has attracted considerable research attention. The short answer is: it depends on the condition, the population, and how guidance is delivered. But for most anxiety and depression presentations, adding a human element consistently moves the needle.
What the Meta-Analytic Evidence Shows
A meta-analysis published in Psychological Medicine examined guidance specifically as a driver of program completion. Guided participants showed a meaningful advantage in finishing their programs, with an effect size of approximately 0.29 Hedges' g (95% confidence interval: 0.18 to 0.40) and completion rates roughly 12 percentage points higher than unguided participants.1 That may sound modest, but in digital mental health, where dropout is a persistent challenge, a 12-point completion gain translates to substantially more people actually receiving a therapeutic dose.
A separate 2022 systematic review and meta-analysis published in JMIR Mental Health, focusing on internet-based self-help for adolescents and college students, found effect sizes in the small-to-moderate range for depression (SMD approximately -0.42), anxiety (-0.35), and stress (-0.35), with quality-of-life improvements of similar magnitude.2 Interventions running longer than eight weeks showed somewhat stronger anxiety outcomes (-0.44 SMD), suggesting that duration interacts with format when estimating benefit.
Condition Matters More Than Many Clinicians Expect
The guidance advantage is most pronounced for depression, where motivation and engagement often erode early in treatment. For insomnia, fully automated digital CBT-I programs have a surprisingly robust track record, and the incremental benefit of adding a human coach appears smaller than in mood disorder applications. Clinicians recommending digital tools should factor in the primary presenting concern rather than assuming that more support is always better.
Who Provides Guidance, and How Often
Not all guidance is equivalent. The parameters that appear to matter most are contact frequency, channel, and provider training. Weekly check-ins tend to outperform on-demand-only contact, and structured asynchronous support via chat or email can be as effective as phone contact for many presentations. A 2026 trial published in Cognitive Behaviour Therapy found that weekly guided and unguided formats produced similarly large within-group effect sizes (around 1.05 to 1.10 Cohen's d) on both depression and anxiety measures,3 suggesting that a well-designed program with weekly structured contact may approach the ceiling of what guidance adds for some populations.
Can Paraprofessional Coaches Substitute for Licensed Clinicians?
For mild-to-moderate cases, the evidence increasingly suggests yes, provided supervision structures are in place. The Newman et al. (2026) Penn State trial used coaches with bachelor's degrees who were enrolled in postgraduate mental health training and received weekly supervision from licensed psychologists. That model produced outcomes that held up over two years. The University of Helsinki's review of CBT-based guided self-help models similarly found that structured lay coaching, when anchored in weekly supervision, can deliver clinically meaningful results without requiring a licensed therapist at every touchpoint.4
For practitioners navigating clinical supervision challenges for new therapists, the paraprofessional model underscores a broader principle: supervision architecture matters as much as who delivers the intervention. The practical implication is that the goal is not replicating traditional therapy inside an app. It is designing a support structure with clear supervision, appropriate case selection, and honest escalation pathways for clients who exceed what self-help formats can safely address.
Guided Vs. Unguided Digital Self-Help: Key Differences
The debate over whether digital self-help requires human support has matured into a practical question of when and how guidance adds value. Data from recent studies reveal that unguided and guided formats achieve strikingly similar symptom reductions for depression and anxiety (effect sizes near 1.1 for both1), but diverge on adherence, resource use, and long-term outcomes.
Clinical Effectiveness and User Engagement
For generalized anxiety, unguided interventions showed a 60% response rate and 45% remission rate, compared to 49% and 37% in guided programs.1 However, real-world adherence to fully self-guided apps remains low: one 2022 study found only 14.8% of users completed all modules, while 68.6% finished fewer than half.2 In controlled trials, both guided and unguided arms achieved equal module completion rates (66%), suggesting that trial environments mask real-world engagement gaps.1 Despite similar symptom improvement, guided programs produce superior diagnostic outcomes at post-treatment and six-month follow-up, along with higher user satisfaction.3
Clinician Time and Resource Allocation
Guided digital self-help requires an average of 66 minutes of clinician time per user, while unguided versions demand roughly 36 minutes.1 That extra half-hour of professional involvement may explain the long-term diagnostic edge and satisfaction boost, but it also reduces scalability. For systems with high demand and limited clinician availability, unguided options can stretch resources further, even if adherence outside structured studies remains a challenge. technology trends in counseling are already reshaping how practitioners weigh these tradeoffs.
Navigating Career and Credentialing Landscapes
Beyond clinical metrics, practitioners weighing these approaches benefit from understanding the professional ecosystem. Job roles differ: guided programs rely on licensed clinicians or supervised coaches, while unguided platforms depend on developers, UX researchers, and content creators. Training pathways likewise diverge; guided roles often require credentials tracked by the American Psychological Association or the National Association of Social Workers, whereas unguided development skills may be verified through a range of technical training channels. employer perceptions of online counseling psychology degrees are still evolving, and searches on Google Scholar or LinkedIn surveys can surface emerging trends for practitioners deciding which pathway to pursue.
Related Articles
Adherence, Dropout, and What Drives Engagement
The single biggest practical challenge with digital self-help therapy is not whether the programs work, but whether people actually finish them. Completion is the gap between a well-designed intervention and a real-world outcome.
The Dropout Problem in Plain Numbers
Recent evidence paints a wide and sometimes sobering picture. A 2024 analysis of digital mental health interventions for adults found median attrition sitting around 18 to 19 percent, with a range running from 5.3 percent to 87 percent depending on the program and population.1 In real-world settings outside controlled trials, attrition figures between 50 and 100 percent are not unusual.2 Unguided self-help programs tend to cluster toward the harder end of that range, with many reporting that fewer than a third of users complete all modules. Guided formats, where a coach or clinician checks in regularly, consistently show better retention. That gap is not trivial. A program that produces strong outcomes in completers may still underperform in practice if most users drop out before reaching a therapeutic dose.
Who Is Most Likely to Stop Early
Attrition is not random. The strongest predictors of early dropout include younger age, higher symptom severity at baseline, low initial motivation, and limited comfort with digital tools. Program-level factors matter just as much: interventions that run long, rely heavily on dense text, or fail to show users meaningful progress tend to lose people faster. This matters for clinical decision-making. Recommending a program based on efficacy data alone, without considering whether a specific patient is likely to engage with it, is only half the job. The mental health workforce shortage makes this calculus especially urgent, since digital tools are often deployed precisely when human capacity is stretched thin.
Design Features That Keep People Engaged
Evidence from the past several years points to a consistent set of features that support adherence. Shorter modules, ideally under 20 minutes each, reduce the friction of starting a session. Push notifications written in a warm, conversational tone rather than generic reminders perform better than standard alerts; research on text-based reminders in mental health programs found they can reduce appointment nonattendance by around 13 percent.2 Gamification elements such as progress bars, streaks, and milestone acknowledgments add low-cost motivation. Adaptive or personalized content, which adjusts based on what a user has already completed or reported, helps the program feel relevant rather than generic. Cultural adaptation also matters more than surface-level translation: programs with deep cultural tailoring show a median dropout rate around 11 percent and a median adherence rate of 75 percent, compared to much wider variance (0 to 56 percent dropout) in programs that only adapt language or visuals.1
The Clinical Takeaway
Efficacy data tells you what a program can do under good conditions. Adherence data tells you what it is likely to do for your patient. When recommending a digital self-help tool, clinicians should factor in the patient's baseline motivation, digital comfort, symptom severity, and available support structures alongside the program's evidence base. The two questions are equally important: does this work, and will this person use it long enough for it to work?
Cost-Effectiveness: How Digital Self-Help Compares to Traditional Therapy
A traditional course of psychotherapy and a digital self-help program can both produce meaningful clinical gains, but they arrive at those gains through very different economic paths. Understanding that gap matters not just for health systems and insurers, but for clinicians deciding how to structure care.
What the Numbers Show
Several economic evaluations published between 2021 and 2026 suggest that digital interventions can deliver strong value relative to their cost. A meta-analysis published in JMIR found that internet-based mental health interventions generated an incremental net benefit of roughly $255 per participant, measured against a willingness-to-pay threshold of $40,000 per quality-adjusted life year.1 The QALY gain was modest, but so was the cost difference, which together placed digital options well within accepted cost-effectiveness ranges.
A 2022 systematic review in Nature offered more granular comparisons. Guided digital self-help showed a 90 percent probability of being cost-effective at a threshold of 30,000 British pounds per QALY, and it dominated control conditions in 64 to 95 percent of probability estimates.2 When stacked against face-to-face CBT, guided digital self-help remained cost-effective in 34 to 79 percent of scenarios, a narrower window that reflects face-to-face therapy's stronger per-person outcomes. Unguided digital self-help for PTSD fared considerably worse, reaching cost-effectiveness in only about 27 percent of scenarios, a reminder that removing human support has real tradeoffs beyond engagement.2
From an employer-facing perspective, the contrast becomes more striking. One analysis placed digital CBT delivery at roughly $30 per user, compared to $600 to $900 for a standard course of traditional psychotherapy.3 In effect-size terms per $1,000 spent, digital CBT generated nearly seven times the output of traditional therapy, though completers of face-to-face therapy still showed a larger absolute effect size (around 0.80 versus 0.96 for digital completers who finished the program).3
The Scalability Argument
The economic case for digital self-help rests heavily on marginal cost. Once a platform is built, adding another user costs almost nothing, whereas every additional therapy client requires another hour of a licensed clinician's time. At a population level, that distinction is significant. The rural mental health services gap and similar coverage shortfalls mean that systems facing long waitlists or under-resourced settings can extend reach without proportionally expanding their workforce.
This is precisely the logic behind the Penn State study led by Michelle Newman, published in 2026, which found that a digital guided CBT platform outperformed traditional therapy referral for over 6,000 college students across 26 campuses. The platform's ability to serve that volume simultaneously would be structurally impossible with therapist-only delivery.
Stepped Care as the Sweet Spot
Cost data alone tends to favor digital tools, but outcomes data complicates the picture enough that most experts land on a blended model. Stepped care starts patients in a lower-intensity digital program and escalates to face-to-face therapy only for those who do not respond. That design captures the efficiency gains of digital delivery while preserving human expertise for cases that need it. Several health system pilots have found this approach optimizes both resource use and outcomes, though long-term data on such models is still accumulating.
What the Data Does Not Capture
Cost-effectiveness analyses rarely account for the full picture. Unused or partially completed program licenses represent wasted spend. Clinician time spent monitoring dashboards, following up on flagged responses, and supervising coaches adds overhead that does not always appear in program-level cost estimates.
Equity concerns deserve equal attention. When cost savings depend on replacing human contact with a digital interface, the populations least likely to benefit are often those with limited internet access, lower digital literacy, or disabilities that affect screen-based interaction. Framing digital self-help as universally cost-effective can obscure the ways those savings are unevenly distributed. Clinicians and systems integrating these tools should weigh affordability against accessibility, not treat them as the same thing.
Risks, Limitations, and When Self-Help Is Not Enough
When is it safer to step a patient away from a self-help app and into intensive professional care? The answer comes down to clinical severity and risk. Digital self-help platforms are built for mild to moderate symptoms, and pushing them beyond that boundary can delay necessary treatment.
When Is Digital Self-Help Not Enough?
Several clinical presentations clearly fall outside the scope of digital self-help. These include: - Active suicidal ideation or recent suicide attempts - Psychosis, including hallucinations or delusions - Severe substance use disorders requiring medical detoxification - Complex PTSD with significant dissociation or self-harm - Acute crisis states, such as recent trauma or manic episodes
For these conditions, immediate professional evaluation and intervention are essential. Recommending a self-help app in such cases can create a false sense of safety while symptoms escalate.
The Risk of Overreliance and Avoidance
Some patients use digital tools as a way to avoid the deeper, more uncomfortable work of therapy. They may cycle through multiple self-help programs, never committing long enough to see change, or substitute app check-ins for genuine emotional processing. Clinicians should be alert to this pattern, especially in patients who repeatedly report "trying everything" yet show no functional improvement. In those cases, the app becomes a form of avoidance rather than a therapeutic adjunct.
Equity, Access, and Cultural Gaps
Not everyone benefits equally from digital self-help. Older adults may struggle with navigation or trust. Rural mental health wait times are already a significant barrier, and unreliable broadband in many rural areas makes video or interactive modules inaccessible on top of that. Low digital literacy cuts across demographics and can turn a supposed low-barrier tool into another obstacle. Moreover, the vast majority of digital self-help programs are designed by and for English-speaking Western populations. They may lack culturally adapted metaphors, examples, or symptom expressions, reducing relevance for many communities. Disability accessibility also remains inconsistent: many apps are not fully compatible with screen readers or alternative input devices, excluding users with visual or motor impairments.
Data Privacy Is a Clinical Concern
When clinicians recommend an app, they implicitly endorse its safety. Yet many consumer mental health apps share user data with advertisers, analytics firms, or social media platforms. Some are not HIPAA compliant, and their privacy policies may be opaque. Practitioners have an ethical obligation to investigate a tool's data practices, including where information is stored, who has access, and whether the company sells or shares data, before integrating it into a treatment plan.
Matching Intervention to Severity
The clinical bottom line is straightforward: digital self-help belongs in a stepped-care model, serving as an entry point or complement for mild-to-moderate presentations. It is not a substitute for professional therapy, medication management, or crisis services. The clinician's role is to assess patient readiness, risk level, and context, then recommend the appropriate intensity of care. Used judiciously, digital self-help extends reach; used carelessly, it can leave high-risk individuals without the support they need.
How Clinicians Can Integrate Digital Self-Help Into Practice
The central challenge is balancing efficiency with individualized care. Digital self-help tools can extend your reach, but only when deployed thoughtfully within a clinical framework that matches intensity of intervention to client need.
Building a Stepped-Care Framework
Digital self-help works best when positioned deliberately within your treatment continuum. Consider these four use cases:
- First step for mild presentations: When a client presents with subthreshold depression or mild anxiety, a structured digital CBT program can serve as initial intervention. If symptoms resolve, you have avoided unnecessary resource use. If they persist or worsen, you escalate to direct therapy with baseline data already collected.
- Bridge during waitlists: Many practices face two to four week gaps before intake. Assigning a specific program during this window keeps clients engaged and provides preliminary skill building. The 2026 Penn State study found that college students randomized to digital guided self-help showed superior outcomes compared to those simply referred to traditional services, partly because treatment began immediately.
- Augmentation between sessions: For clients in active therapy, digital modules can reinforce session content. A client working on social anxiety might complete exposure hierarchy modules between appointments, freeing session time for processing rather than psychoeducation.
- Relapse prevention after discharge: Booster modules help maintain gains. Clients can revisit behavioral activation or cognitive restructuring content during vulnerable periods without requiring a full return to care.
Practical Integration Moves
Vague recommendations produce vague results. Instead of suggesting a client "try an app," prescribe a specific program by name and explain why it fits their presentation. Set clear expectations: "Complete modules one through three before our next session" creates accountability. Schedule brief check-ins, whether by secure message or phone, to review progress and troubleshoot barriers. When programs generate usage data or symptom tracking, incorporate that information into session planning. Thinking ahead about technology trends in counseling can help you evaluate which platforms are likely to remain viable and evidence-informed over time.
Scope-of-Practice Considerations
Recommending a self-help tool falls within scope for LMFTs, LCSWs, CMHCs, and psychologists alike. However, the clinical decision-making around when to escalate care differs by training and setting. Psychologists may be positioned to interpret screening data and adjust diagnostic formulations independently. Social workers and counselors practicing in agency settings may need to consult with supervisors or refer out when presentations exceed program parameters. Understanding clinical supervision hours for licensure requirements in your state is especially relevant here, since documentation of your reasoning around digital tool use may intersect with supervised practice standards. Know your state regulations and document your clinical reasoning when adding or discontinuing digital tools.
Try It Before You Recommend It
Spend 20 minutes walking through a module before assigning it to any client. This builds credibility when you discuss the program and lets you anticipate questions or confusion points. You will also discover whether the content aligns with your theoretical orientation and client population. A program designed for college students may not translate well to older adults, and you will only notice this by engaging with the material yourself.
Evaluating Digital Self-Help Tools: A Checklist for Practitioners
Before recommending or integrating any digital self-help platform into your practice, run it through these six evaluation criteria. A tool that checks every box is not guaranteed to work for every client, but skipping any of these areas introduces avoidable risk.
- Evidence QualityDetermine whether the specific program, not just the broader therapeutic modality it draws from, is supported by at least one published randomized controlled trial in a peer-reviewed journal. A platform built on CBT principles, for example, is not the same as one whose own version of CBT-based modules has been independently tested. Look for studies that report effect sizes, follow-up duration, and clinically meaningful outcomes rather than satisfaction surveys alone.
- Regulatory and Classification StatusUnderstand what category the tool falls into: an FDA-cleared digital therapeutic, a research-grade platform used in clinical trials, or a consumer wellness app with no regulatory oversight. The distinction shapes how much clinical weight you can place on it. An FDA-cleared product has met specific safety and efficacy thresholds; a wellness app may not have undergone any formal evaluation. Match the classification to your use case, recommending an unregulated app as a standalone treatment carries different liability than using a cleared tool as an adjunct.
- Data Privacy and HIPAA ComplianceIf you are using the platform within a clinical context, confirm that it complies with HIPAA requirements for protected health information. Beyond compliance, review whether the platform shares user data with third parties, what data it collects beyond clinical inputs, and whether its privacy policy is transparent and accessible to clients. A tool that monetizes user data or lacks clear data-handling protocols is a liability regardless of its clinical effectiveness.
- Cultural and Linguistic AdaptationCheck whether the program is available in the languages your clients speak and whether it has been validated in populations that reflect your caseload's demographic diversity. A program tested exclusively in English-speaking college students, such as the large-scale trial by Newman and colleagues at Penn State, may not generalize to older adults, non-English speakers, or communities with different cultural frameworks around mental health. Validation in diverse samples strengthens your confidence in recommending it broadly.
- Usability and AccessibilityEvaluate whether the interface is navigable for clients with varying levels of digital literacy. At minimum, the platform should meet basic accessibility standards: screen reader compatibility, adjustable text size, and intuitive navigation. If a client cannot use the tool independently or finds it frustrating, adherence will suffer regardless of how strong the evidence base is. When possible, walk through the platform yourself before recommending it.
- Guidance Model and Crisis SafetyClarify whether the platform is fully self-directed, offers human coaching, or includes features that allow integration with a clinician's workflow. Research consistently shows that guided digital self-help produces stronger outcomes than unguided versions, so the presence or absence of a support structure matters. Equally important, verify that the platform has crisis safety protocols, clear pathways to emergency resources if a user reports suicidal ideation or acute distress. A tool without safety netting should not be used with higher-risk populations.
Frequently Asked Questions About Digital Self-Help Therapy
Clinicians exploring digital self-help therapy often share a common set of questions about efficacy, appropriate use, and practical integration. The answers below draw on current research, including the 2026 Newman et al. study of over 6,200 college students, to address the most frequent concerns raised by practitioners across counseling, clinical psychology, social work, and related fields.