What you’ll learn in this article…
- Most suicide counselor roles require a master's degree plus 2,000 to 4,000 supervised clinical hours post-graduation.
- The full path from college enrollment to specialized certification typically spans 8 to 12 years.
- BLS projects 22% job growth for mental health counselors between 2022 and 2032, far exceeding the national average.
- Key suicide-specific credentials include CAMS, QPR Gatekeeper, CALM, and the AAS Crisis Specialist designation.
Suicide is the 11th leading cause of death in the United States, claiming more than 47,000 lives annually, and trained specialists who can intervene before a crisis becomes fatal are consistently in short supply. That demand is real, but so is the credentialing barrier: most clinical positions require a master's degree, thousands of supervised hours, and a state license before a counselor can work independently with high-risk clients.
A suicide counselor is a licensed mental health professional who specializes in suicide risk assessment, crisis intervention, and ongoing treatment for individuals experiencing suicidal ideation or behavior. The role is distinct from general crisis counseling, and the path to it is longer and more structured than many prospective students expect.
The field is not static. Specialty certifications, telehealth crisis lines, and expanded crisis center funding are reshaping where and how this work happens, making the decision about which degree, license, and certification to pursue more consequential than ever.
What Is a Suicide Counselor?
What exactly does a suicide counselor do, and how is this role different from other crisis intervention professionals?
A suicide counselor is a licensed or credentialed mental health professional who specializes in working with individuals experiencing suicidal thoughts, urges, or behaviors. The core responsibilities include conducting comprehensive suicide risk assessments, developing personalized safety plans, and providing both immediate crisis intervention and longer-term therapeutic support. Unlike general mental health practitioners who may encounter suicidal clients occasionally, suicide counselors focus their clinical practice specifically on suicide prevention and postvention care.
Core Responsibilities
Suicide counselors perform specialized clinical functions that require advanced training beyond standard counseling education:
- Risk assessment: Evaluating the severity and immediacy of suicidal ideation using validated screening tools and clinical interviews
- Safety planning: Collaborating with clients to create detailed, actionable plans that identify warning signs, coping strategies, and emergency contacts
- Therapeutic intervention: Delivering evidence-based treatments designed specifically for suicidal individuals, such as Dialectical Behavior Therapy or Cognitive Behavioral Therapy for suicide prevention
- Means restriction counseling: Working with clients and families to reduce access to lethal methods during high-risk periods
- Postvention support: Providing care to suicide attempt survivors and those bereaved by suicide loss
How This Role Differs from Adjacent Positions
Suicide counseling is often confused with related roles, but important distinctions exist.
Crisis hotline workers typically function as paraprofessionals who provide immediate phone-based support following structured protocols. They complete focused training programs lasting 40 to 80 hours and work primarily through text, chat, or voice contact. In contrast, suicide counselors hold graduate degrees, maintain clinical licenses, and provide ongoing face-to-face therapeutic relationships. For a broader look at this adjacent career path, see our guide on how to become a crisis intervention specialist.
Licensed therapists with general practices address a broad range of mental health concerns, from anxiety and depression to relationship issues and trauma. While they may encounter suicidal clients, their training in suicide-specific assessment and intervention varies widely. Suicide counselors dedicate their practice to this population and pursue specialized certifications.
Peer specialists bring invaluable lived experience with suicidal crises or mental health challenges. They offer support, share recovery strategies, and help clients navigate systems of care. However, they do not conduct clinical assessments, diagnose conditions, or provide psychotherapy.
Professional Credentials and Settings
It is important to understand that "suicide counselor" describes a specialization within clinical counseling rather than a standalone license. Practitioners typically hold credentials such as Licensed Professional Counselor, Licensed Clinical Social Worker, Licensed Mental Health Counselor, or Licensed Marriage and Family Therapist. They then pursue additional suicide-specific training through programs like the Collaborative Assessment and Management of Suicidality or certifications from the American Association of Suicidology.
You will find professionals using this title in several settings: 988 Suicide and Crisis Lifeline centers, hospital psychiatric units and emergency departments, Veterans Affairs facilities, community mental health agencies, and specialized outpatient clinics. In each of these environments, the focus remains consistent: reducing suicide risk through expert clinical intervention and compassionate, evidence-based care.
Suicide Counselor Vs. Crisis Counselor: Key Differences
While suicide counselors and crisis counselors share the goal of immediate emotional support, they differ in focus, training, and scope.1 Understanding these distinctions helps aspiring professionals choose the right path.
Defining the Roles
Suicide counselors specifically address suicidal ideation and behavior. They conduct risk assessments, de-escalate acute crises, and create safety plans to prevent self-harm. Their role is deeply embedded in suicide prevention frameworks. In contrast, crisis counselors provide broader brief interventions for a range of emergencies, including trauma, grief, and mental health crises.1 Their work focuses on stabilizing the individual, offering coping strategies, and connecting them to longer-term resources.
Scope of Practice and Session Structure
The practical differences are significant:
- Primary function: Suicide counselors center on suicide prevention, while crisis counselors aim for immediate stabilization and referral.1
- Session length: Suicide counseling sessions are typically brief, focused on imminent safety. Crisis counseling may extend from 15 minutes to two hours across one to three sessions.2
- Work format: Both may work on hotlines or chat platforms, but suicide counselors are more often embedded in dedicated suicide prevention lines or crisis response teams. Crisis counselors additionally offer face-to-face and trauma response services.
Education and Training Pathways
Educational requirements diverge. Suicide counselors usually need a master's degree in counseling, social work, or a related field, along with specialized training in suicide assessment models like CAMS or ASIST.1 Crisis counselors can enter the field with a bachelor's degree, though many hold master's degrees as well. This makes crisis counseling a more accessible entry point, while suicide counseling typically requires advanced clinical training for the intensity and complexity of the work. Those interested in the broader crisis field can explore becoming a crisis intervention counselor.
Work Settings and Compensation
Both professionals are found in community mental health centers, hospitals, and crisis hotlines. However, suicide counselors may additionally work within school systems, correctional facilities, or the military, where suicide prevention is a mandated priority. Professionals interested in that military pathway may want to learn about the army behavioral health specialist role. Compensation data for suicide counselors is not separately reported in national wage surveys.1 By comparison, crisis counselors earned a mean annual wage of $65,100 in 2024 according to available data, though earnings can vary widely by location, employer, and education level. Those with master's degrees and clinical licenses are likely to command higher salaries.
Education Requirements by Role and Degree Level
Most suicide counselor positions require a master's degree in counseling, social work, or psychology, along with 2,000 to 4,000 hours of supervised clinical experience post-graduation. That timeline and credential burden define the standard clinical entry point, but several other pathways exist depending on the scope of work you intend to pursue.
Associate Degree: Paraprofessional and Crisis-Line Roles (≈2 years)
An associate degree in human services, psychology, or a related field can qualify you for paraprofessional positions such as crisis hotline volunteer coordinator, peer support specialist trainee, or intake assistant at community mental health centers. These roles typically do not involve independent clinical assessment or therapy, but they provide foundational crisis-intervention training and exposure to suicide prevention protocols. Many national crisis hotlines accept volunteers with high school diplomas and provide in-house training, so an associate degree is not always mandatory for entry-level crisis work.
Bachelor's Degree: Case Management and Peer Specialist Roles (≈4 years)
A bachelor's degree in psychology, social work, or a related behavioral science opens doors to case manager, peer specialist, and crisis intervention aide positions. In these roles, you may conduct safety planning, coordinate referrals, and provide follow-up support under licensed supervision. While you cannot independently diagnose or provide therapy, you can accumulate valuable fieldwork hours and determine whether graduate-level clinical training aligns with your career goals. Some states credential peer specialists separately, especially those with lived experience of mental health challenges.
Master's Degree: Licensed Clinical Practice (≈6-7 years total)
A master's degree in clinical mental health counseling, social work (MSW), or marriage and family therapy is the practical minimum for independent suicide counseling work. After completing a 60-credit master's program (typically two years full-time), you must accumulate 2,000 to 4,000 hours of supervised clinical practice, depending on state licensure requirements, before sitting for the licensed professional counselor (LPC), Licensed Clinical Social Worker (LCSW), or Licensed Mental Health Counselor (LMHC) examination. This supervised period usually takes two to three additional years. Tuition for master's programs ranges from approximately $20,000 at public universities to $60,000 or more at private institutions, with online and hybrid formats often falling in the mid-range. Many community mental health counselor employers offer loan repayment assistance or Public Service Loan Forgiveness eligibility, offsetting the upfront cost for clinicians willing to work in underserved settings.
Doctoral Degree: Psychologist, Researcher, Suicidologist (≈8-10 years total)
A Ph.D. or Psy.D. in clinical or counseling psychology prepares you for advanced clinical roles, supervision, academic research, and specialized suicidology positions. Doctoral training includes dissertation research, comprehensive exams, and a full-time predoctoral internship. Licensed psychologists can conduct psychological testing, provide expert testimony, and design evidence-based suicide prevention interventions. If you are drawn to research, program evaluation, or policy development, a doctorate offers the credentialing and methodological training to lead large-scale prevention initiatives.
What Degree Do You Need to Be a Suicide Prevention Counselor?
For independent clinical practice, a master's degree in counseling, social work, or psychology is the standard requirement. Bachelor's and associate degrees qualify you for support and paraprofessional roles, while a doctorate is necessary only for advanced research, supervision, or licensed psychologist positions. The master's-plus-licensure pathway remains the most common route into full-time suicide counseling careers. For a broader overview of the counseling profession, see our guide on how to become a counselor.
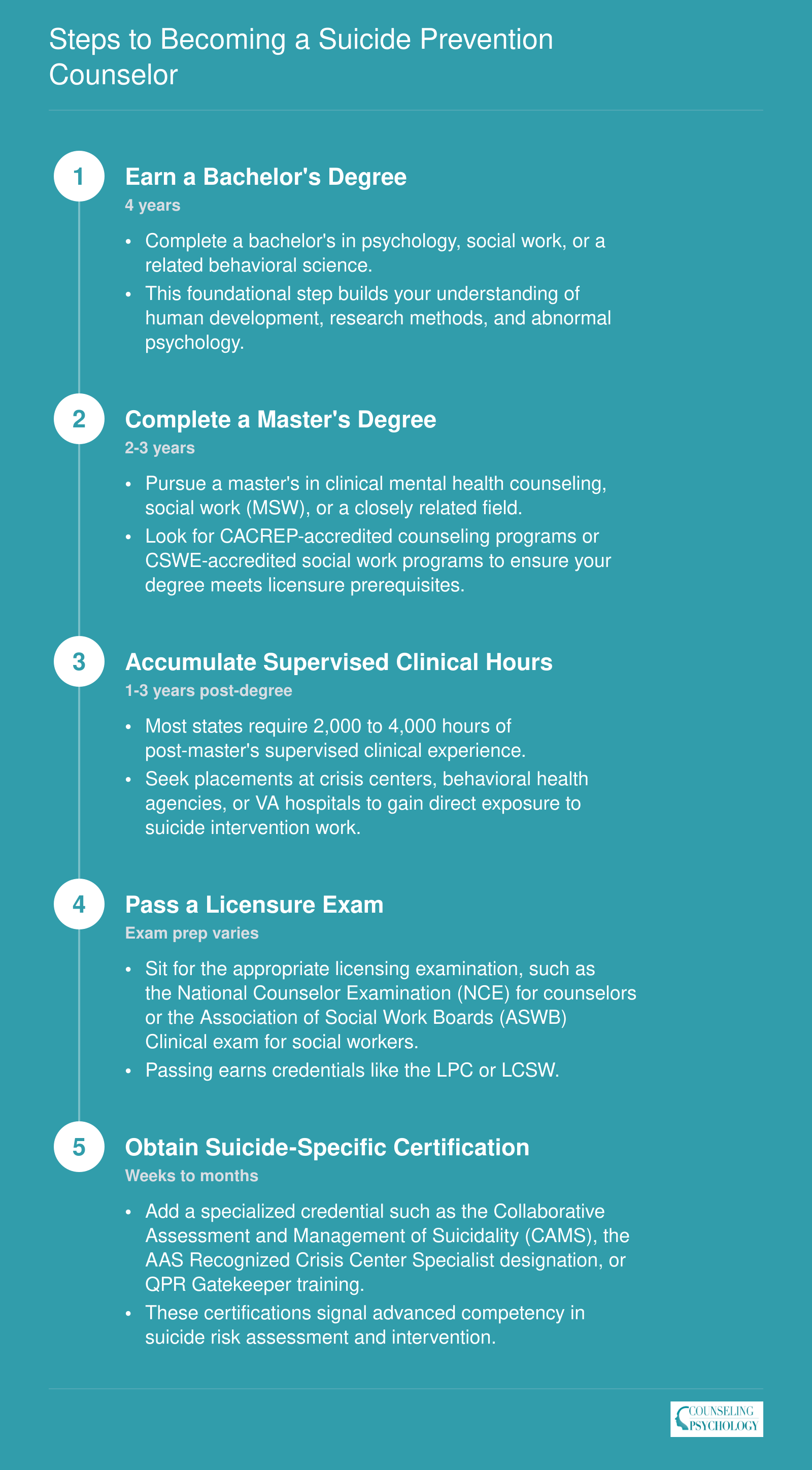
Steps to Becoming a Suicide Prevention Counselor
From your first college course to a specialized credential, the path to becoming a suicide prevention counselor typically spans 8 to 12 years of education, supervised practice, and certification. Here is the credentialing ladder most professionals follow.
Licensure and Certification Pathways
A clinical license is the legal gateway to independent suicide counseling practice, and the specific credential you pursue shapes where and how you can work with high-risk clients. Four main licenses dominate the mental health landscape, each with distinct requirements and workplace advantages.
Core Clinical Licenses
- Licensed Professional Counselor (LPC): Requires a master's degree in counseling, passage of the National Counselor Examination (NCE) or National Clinical Mental Health Counseling Examination (NCMHCE), and typically 2,000 to 4,000 hours of supervised clinical experience. LPCs frequently staff community mental health centers and crisis hotlines where suicide intervention is routine.
- Licensed Clinical Social Worker (LCSW): Requires a Master of Social Work (MSW) from a CSWE-accredited program, the Association of Social Work Boards (ASWB) Clinical exam, and approximately 3,000 supervised hours in most states. LCSWs dominate hospital emergency departments, Veterans Affairs settings, and integrated care teams responding to suicidal patients.
- Licensed Mental Health Counselor (LMHC): Used in states like New York and Florida, this credential mirrors LPC requirements: a master's in counseling, a national exam, and 2,000 to 3,000 supervised hours. Those interested in the full pathway can explore how to become a mental health counselor for a deeper breakdown. LMHCs often work in outpatient clinics and private practices specializing in mood disorders and trauma.
- Licensed Marriage and Family Therapist (LMFT): Requires a master's degree emphasizing relational therapy, passage of the MFT National Examination, and around 3,000 supervised hours. LMFTs are well positioned for adolescent suicide prevention work within family therapy practices and school-based programs. A detailed overview of the LMFT track is available in our guide on how to become a marriage and family therapist.
Suicide-Specific Certifications as Add-On Credentials
Once you hold a clinical license, suicide-specific certifications deepen your specialization and signal advanced competency to employers. These credentials do not replace licensure but function as evidence-based skill endorsements that improve employability at crisis centers, hospitals, and specialized outpatient programs.
How Long Does Crisis Intervention Certification Take?
Timelines vary dramatically depending on the credential's depth. QPR Gatekeeper training, designed as a basic awareness program, can be completed in one to two hours. More rigorous credentials like the Collaborative Assessment and Management of Suicidality (CAMS) framework require several months of structured training, supervised case consultation, and demonstration of fidelity to the model. Intermediate options like Applied Suicide Intervention Skills Training (ASIST) typically involve a two-day workshop. Prospective suicide counselors should view these certifications as progressive layers: entry-level programs build foundational awareness, while advanced credentials like CAMS or the American Association of Suicidology's Crisis Specialist certification establish clinical expertise that distinguishes candidates in competitive job markets.
Comparing Suicide-Specific Certifications: CAMS, QPR, CALM, and AAS Crisis Specialist
Four specialized certifications stand out in suicide prevention work: CAMS (Collaborative Assessment and Management of Suicidality), QPR Gatekeeper, CALM (Counseling on Access to Lethal Means), and the American Association of Suicidology Recognized Crisis Worker or Crisis Center Specialist credential. Each targets a distinct skill set and audience, with varying prerequisites, training durations, and renewal requirements. Understanding these differences helps practitioners choose credentials that align with their career goals and practice settings.
Where to Find Certification Details
Each certifying body maintains official websites with current requirements, fees, and application instructions. For CAMS, the CAMS-Care website publishes training schedules, prerequisite qualifications (typically a master's degree and clinical licensure), and costs. QPR Institute offers its Gatekeeper training details directly on qprinstitute.com, including options for individual certification and trainer-of-trainers models. The CALM certification, developed by researchers at Harvard and disseminated through multiple partner organizations, is documented at sites affiliated with the Means Matter campaign and Suicide Prevention Resource Center. The American Association of Suicidology (suicidology.org) lists criteria for its Recognized Crisis Worker and Crisis Center Specialist credentials, which focus on hotline and crisis center staff.
Evaluating Prerequisites and Commitment
Certifications differ sharply in their entry requirements. CAMS training is designed for licensed mental health professionals, such as clinical psychologists, licensed professional counselors, and clinical social workers, who already hold graduate degrees and active state licenses. QPR Gatekeeper, by contrast, is accessible to anyone interested in suicide prevention, from teachers and coaches to clergy and community volunteers, with no formal mental health education required. CALM training typically targets clinicians and public health professionals who work with at-risk populations but may not require full licensure. AAS credentials focus on crisis intervention experience rather than academic degrees, making them well suited to hotline workers and peer support specialists.
Understanding Training Duration and Renewal
Training length ranges from one-hour online modules to multi-day intensive workshops. QPR Gatekeeper certification can be completed in 90 minutes, while CAMS requires a full-day or multi-session workshop with ongoing consultation and fidelity monitoring for those using the protocol clinically. CALM training typically spans several hours and emphasizes counseling on firearm and medication safety. AAS credentials involve documented crisis intervention hours and supervised experience, with renewal requirements tied to continuing education in crisis and suicide-specific topics. Check each organization's website for current renewal cycles, which may range from annual to multi-year intervals, and associated costs.
Aligning Credentials with Career Goals
Choosing the right certification depends on your role, setting, and scope of practice. Licensed clinicians providing direct therapy often pursue CAMS to integrate evidence-based suicide assessment into their clinical workflow. Community gatekeepers, educators, and first responders frequently select QPR for its brevity and broad applicability. Providers in emergency departments, primary care, or public health roles may prioritize CALM to address lethal means counseling. Crisis center staff and hotline counselors benefit from AAS credentials that validate their specialized training and experience; those interested in broader crisis work may also explore crisis intervention specialist certification. Professional associations such as the American Association of Suicidology and the National Action Alliance for Suicide Prevention offer additional guidance on matching credentials to practice contexts.
Skills, Competencies, and Emotional Readiness
Effective suicide counseling demands a specific blend of clinical expertise, interpersonal skills, and psychological resilience. Beyond academic credentials and certifications, practitioners must develop competencies that allow them to engage safely and therapeutically with clients experiencing acute suicidal distress.
Core Clinical Competencies
Four foundational skills distinguish proficient suicide counselors from mental health counselor generalists:
- Lethal means assessment: Systematically evaluating a client's access to firearms, medications, and other methods. The Counseling on Access to Lethal Means (CALM) training teaches counselors to conduct these conversations with sensitivity while reducing immediate risk.
- Collaborative safety planning: Using the Stanley-Brown Safety Planning Intervention, counselors work alongside clients to identify warning signs, internal coping strategies, social supports, and environmental safety modifications. This brief, structured approach is now standard in emergency departments, outpatient clinics, and crisis settings.1
- Risk formulation: Moving beyond simple checklists to synthesize historical, clinical, and contextual factors into a coherent understanding of why a person is suicidal now. The Collaborative Assessment and Management of Suicidality (CAMS) framework provides a structured method for identifying and addressing the unique drivers of each individual's suicidal state.1
- De-escalation and cognitive restructuring: Drawing from Dialectical Behavior Therapy (DBT) for emotion regulation and distress tolerance, as well as Cognitive Behavioral Therapy for Suicide Prevention (CBT-SP) for restructuring hopeless thought patterns, counselors learn to reduce acute distress while building longer-term coping capacity.1
Emotional Readiness and Self-Awareness
Working with suicidal clients requires comfort with ambiguity. Not every intervention will produce a clear positive outcome, and counselors must tolerate uncertainty without becoming paralyzed or overly controlling. Equally important is the ability to recognize and manage countertransference, the emotional reactions that arise when a client's distress triggers personal memories or anxieties.
Practitioners should also expect documentation-heavy workflows. Crisis work involves detailed risk assessments, safety plans, and coordination notes. Those who find extensive paperwork frustrating may struggle with the administrative demands inherent to these roles.
Burnout, Vicarious Trauma, and Self-Care as Professional Practice
Crisis counselors face elevated risks of burnout, compassion fatigue, and secondary traumatic stress.1 Compassion fatigue combines the exhaustion of burnout with the intrusive symptoms of vicarious trauma, creating a particularly challenging occupational hazard.2 Tools like the Professional Quality of Life Scale (ProQOL) help practitioners monitor their own compassion satisfaction alongside burnout and secondary traumatic stress levels.
Research confirms that mental health professionals working with traumatized populations experience significant rates of secondary traumatic stress symptoms.1 Self-care is not optional in this field. It functions as a professional competency rather than a personal indulgence.
SAMHSA's guidance for crisis counselors emphasizes concrete mitigation strategies: regular peer support and consultation, adequate sleep and exercise, scheduled breaks during shifts, and consistent check-ins with clinical supervisors.2 Many practitioners also maintain their own therapy relationships to process the emotional weight of the work.
Employer Expectations for Self-Care Planning
Recognizing these occupational risks, many crisis-focused employers now require demonstrated self-care plans as part of the onboarding process. New hires may be asked to articulate their personal strategies for maintaining wellness, identify their support networks, and commit to caseload boundaries. Organizations increasingly view these plans as essential infrastructure for sustainable crisis services, not as bureaucratic formalities. Counselors who proactively develop these habits position themselves for longer, healthier careers in this demanding specialty.
Where Suicide Counselors Work
Choosing where to work as a suicide counselor often means weighing the intensity of direct crisis intervention against the stability of a structured organizational setting. The setting shapes your daily tasks, the populations you serve, and even the pace of your career growth. Below are six primary environments where suicide prevention specialists make an impact, each with distinct expectations and rewards.
988 Suicide and Crisis Lifeline Centers
For many aspiring crisis counselors, 988 centers are the most immediate entry point. The national network, administered by Vibrant Emotional Health and funded by SAMHSA, includes over 200 local centers launched in 2022.1 While there is no national degree requirement, qualifications vary by center.2 Many call centers hire bachelor's-level counselors who complete in-house training, while clinical roles, such as mobile crisis response or supervisory positions, typically require a master's degree and state licensure. Aspiring hotline workers often ask about compensation: yes, most 988 crisis counselor positions are paid, though some centers also maintain trained volunteer roles for paraprofessional support.2 Each center develops its own training curriculum, and a core clinical curriculum with interactive simulations launched in November 2022.3 Optional certification through the American Association of Suicidology's Crisis Specialist program is also available to deepen expertise, with recertification required every three years and an exam pass rate of 80%.4
Hospital Emergency Departments and Inpatient Psychiatric Units
Hospitals offer the highest-acuity settings, where suicide counselors work alongside medical staff during psychiatric emergencies. In emergency departments, you perform rapid risk assessments and coordinate inpatient admissions. Inpatient units involve longer-term stabilization, group therapy, and discharge planning. These roles almost always require a master's degree in counseling, social work, or psychology and full clinical licensure. The fast pace and interdisciplinary collaboration make hospital settings ideal for those who thrive under pressure and want to work at the intersection of mental and physical health.
VA Medical Centers and Community Mental Health Agencies
Veterans Affairs medical centers are major employers of suicide prevention coordinators and counselors, serving a population with disproportionately high suicide risk. VA positions often require a master's degree and licensure, and they frequently offer significant loan repayment incentives through federal programs. Similarly, community mental health agencies and federally qualified health centers provide safety-net services and can serve as a launchpad for early-career counselors. These agencies often hire master's-level clinicians and may qualify for state or federal loan forgiveness, making them financially attractive despite lower salaries compared to private practice.
Schools, Private Practice, and Telehealth Platforms
K-12 schools and college counseling centers are increasingly adding suicide prevention specialists to their wellness teams. School-based roles typically require a master's degree in school counseling or a related field, along with state certification; you can learn more about the pathway in our guide on how to become a school counselor. In private practice, licensed counselors can specialize in suicidality and set their own caseloads, though building a referral base takes time. A notable post-pandemic shift is the rapid growth of telehealth-based crisis counseling. Platforms now connect licensed therapists with clients in crisis via video or chat, offering flexibility and geographic reach. This emerging setting is particularly suited for those who value autonomy and want to reach underserved rural areas without relocating.
Suicide Counselor Salary: National Overview
Because the Bureau of Labor Statistics does not track suicide counselors as a standalone occupation, the closest federal benchmark falls under Substance Abuse, Behavioral Disorder, and Mental Health Counselors (SOC 21-1018). This category encompasses many professionals who deliver suicide prevention services, crisis intervention, and behavioral health counseling. The national figures below reflect approximately 440,380 employed workers in this group.
| Wage Metric | Annual Amount |
|---|---|
| National Median Salary | $59,190 |
| 25th Percentile | $47,170 |
| National Mean (Average) Salary | $65,100 |
| 75th Percentile | $76,230 |
Suicide Counselor Salary by State
Because the BLS does not track suicide counselors as a standalone occupation, the figures below come from the broader Substance Abuse, Behavioral Disorder, and Mental Health Counselors category (SOC 21-1018). Salaries vary widely by state, with median annual wages ranging from roughly $47,000 in Mississippi to over $79,000 in Alaska. Professionals holding suicide-specific certifications or working in high-demand crisis settings may earn above these median benchmarks.
| State | Total Employment | 25th Percentile | Median Annual Wage | 75th Percentile | Mean Annual Wage |
|---|---|---|---|---|---|
| Alaska | 1,060 | $63,690 | $79,220 | $96,940 | $88,870 |
| New Mexico | 2,070 | $55,060 | $70,770 | $80,840 | $71,010 |
| Oregon | 6,410 | $56,290 | $69,660 | $84,970 | $72,860 |
| North Dakota | 1,180 | $50,810 | $66,450 | $75,120 | $68,220 |
| District of Columbia | 980 | $47,980 | $66,140 | $83,040 | $71,200 |
| Utah | 4,720 | $42,210 | $65,920 | $94,630 | $71,890 |
| Idaho | 2,130 | $48,570 | $65,240 | $78,100 | $65,290 |
| New Jersey | 14,640 | $51,170 | $64,710 | $84,690 | $75,900 |
| Nebraska | 1,980 | $46,900 | $64,410 | $81,210 | $66,690 |
| Washington | 13,150 | $52,070 | $64,220 | $80,440 | $70,230 |
| Arizona | 8,970 | $50,650 | $63,830 | $79,990 | $67,890 |
| Connecticut | 6,470 | $49,120 | $62,960 | $77,610 | $66,920 |
| Wisconsin | 9,450 | $50,870 | $62,470 | $77,800 | $70,180 |
| New York | 22,450 | $50,880 | $62,070 | $76,680 | $69,290 |
| Wyoming | 840 | $42,610 | $61,640 | $79,830 | $65,650 |
| California | 63,110 | $47,650 | $61,310 | $90,370 | $72,530 |
| Maine | 1,610 | $48,360 | $60,970 | $73,510 | $64,050 |
| Iowa | 3,030 | $49,170 | $60,880 | $78,830 | $65,960 |
| Texas | 19,520 | $47,600 | $60,630 | $76,390 | $67,920 |
| Vermont | 1,150 | $52,890 | $60,410 | $67,670 | $63,060 |
| Illinois | 18,170 | $47,640 | $59,570 | $81,250 | $69,010 |
| Michigan | 11,090 | $42,480 | $59,530 | $74,360 | $61,960 |
| Nevada | 2,240 | $46,960 | $59,470 | $76,260 | $64,430 |
| Colorado | 13,670 | $47,750 | $59,190 | $78,350 | $66,280 |
| Massachusetts | 17,950 | $47,120 | $59,030 | $73,000 | $64,020 |
| Minnesota | 7,910 | $49,880 | $58,720 | $64,370 | $59,020 |
| Montana | 1,900 | $39,220 | $58,660 | $68,360 | $57,350 |
| Oklahoma | 4,460 | $44,320 | $58,610 | $78,710 | $62,220 |
| New Hampshire | 3,100 | $48,310 | $58,520 | $73,770 | $61,100 |
| Virginia | 16,860 | $47,530 | $58,410 | $76,530 | $63,630 |
| Pennsylvania | 26,510 | $46,910 | $58,320 | $72,800 | $61,040 |
| Maryland | 8,180 | $48,980 | $57,820 | $70,990 | $68,830 |
| Kansas | 2,410 | $45,050 | $57,760 | $67,540 | $59,530 |
| Ohio | 16,690 | $47,370 | $56,990 | $67,470 | $59,960 |
| Florida | 24,680 | $46,640 | $56,830 | $67,700 | $60,480 |
| Missouri | 7,500 | $42,930 | $56,640 | $66,810 | $58,230 |
| North Carolina | 8,930 | $47,460 | $56,470 | $68,470 | $60,440 |
| Georgia | 8,680 | $46,150 | $55,320 | $71,980 | $61,250 |
| Hawaii | 1,580 | $49,630 | $54,390 | $76,220 | $75,610 |
| South Dakota | 1,510 | $46,260 | $53,400 | $59,770 | $55,890 |
| Kentucky | 8,030 | $39,560 | $51,790 | $75,310 | $58,190 |
| South Carolina | 4,680 | $40,480 | $50,720 | $65,770 | $55,450 |
| Arkansas | 2,860 | $37,280 | $49,990 | $69,630 | $58,960 |
| Rhode Island | 1,560 | $42,550 | $49,770 | $67,370 | $58,860 |
| Delaware | 1,240 | $41,630 | $49,680 | $65,270 | $56,120 |
| Indiana | 10,400 | $41,860 | $49,280 | $62,780 | $54,630 |
| Alabama | 3,340 | $40,480 | $48,880 | $58,540 | $52,120 |
| Tennessee | 7,310 | $36,910 | $48,170 | $60,900 | $51,480 |
| Mississippi | 2,220 | $37,830 | $46,810 | $56,800 | $54,120 |
Highest-Paying Metro Areas for Suicide and Crisis Counselors
Geography plays a significant role in earning potential for suicide and crisis counselors. The BLS tracks salary data for the broader category of Substance Abuse, Behavioral Disorder, and Mental Health Counselors, which includes professionals focused on suicide prevention and crisis intervention. The metro areas below rank highest by median annual wage, though it is worth noting that higher pay often correlates with a higher cost of living.
| Metro Area | Total Employment | Median Annual Wage | 25th Percentile | 75th Percentile | Mean Annual Wage |
|---|---|---|---|---|---|
| San Francisco, Oakland, Fremont, CA | 8,080 | $72,950 | $54,110 | $108,410 | $83,140 |
| Portland, Vancouver, Hillsboro, OR/WA | 3,640 | $71,530 | $60,230 | $86,150 | $75,920 |
| Sacramento, Roseville, Folsom, CA | 3,570 | $69,510 | $48,860 | $99,790 | $78,880 |
| Seattle, Tacoma, Bellevue, WA | 7,040 | $65,290 | $53,890 | $81,230 | $71,930 |
| New York, Newark, Jersey City, NY/NJ | 23,790 | $64,900 | $52,770 | $81,680 | $75,500 |
| Houston, Pasadena, The Woodlands, TX | 4,230 | $64,140 | $49,340 | $76,890 | $68,820 |
| Phoenix, Mesa, Chandler, AZ | 6,830 | $63,990 | $50,190 | $82,350 | $67,740 |
| Washington, Arlington, Alexandria, DC/VA/MD/WV | 7,590 | $63,170 | $50,280 | $83,780 | $73,210 |
| Chicago, Naperville, Elgin, IL/IN | 14,010 | $61,150 | $47,980 | $83,770 | $70,920 |
| Minneapolis, St. Paul, Bloomington, MN/WI | 4,610 | $60,540 | $50,480 | $68,440 | $61,530 |
| Riverside, San Bernardino, Ontario, CA | 5,170 | $60,860 | $47,490 | $78,210 | $66,800 |
| Boston, Cambridge, Newton, MA/NH | 10,980 | $60,780 | $48,320 | $74,300 | $65,330 |
| Philadelphia, Camden, Wilmington, PA/NJ/DE/MD | 12,860 | $59,990 | $48,610 | $76,700 | $65,190 |
| Columbus, OH | 3,630 | $59,110 | $49,100 | $71,950 | $62,750 |
| Denver, Aurora, Centennial, CO | 6,670 | $59,100 | $48,900 | $74,860 | $66,000 |
| Los Angeles, Long Beach, Anaheim, CA | 23,330 | $58,880 | $47,210 | $84,030 | $69,630 |
| Atlanta, Sandy Springs, Roswell, GA | 5,510 | $58,990 | $48,400 | $73,630 | $64,030 |
| San Diego, Chula Vista, Carlsbad, CA | 5,010 | $58,690 | $47,530 | $79,380 | $68,560 |
| Pittsburgh, PA | 5,400 | $58,760 | $47,750 | $70,510 | $60,970 |
| Miami, Fort Lauderdale, West Palm Beach, FL | 7,610 | $58,200 | $48,380 | $65,430 | $60,330 |
Job Outlook and Career Advancement
The demand for suicide prevention expertise is climbing as mental health infrastructure expands across the United States. Between 2022 and 2032, the Bureau of Labor Statistics projects that employment of substance abuse, behavioral disorder, and mental health counselors will grow 18 percent, significantly faster than the 3 percent average for all occupations.1 This expansion is expected to create 69,500 new positions, with approximately 42,000 annual openings arising from both growth and replacement needs.1
Why Demand Is Accelerating
Three structural forces are driving this surge. First, the expansion of the 988 Suicide and Crisis Lifeline has created a nationwide network of crisis centers that require trained staff around the clock. Second, federal and state funding streams have widened: provisions in the Bipartisan Safer Communities Act of 2022 allocated hundreds of millions of dollars for school-based mental health services and community crisis response, much of it earmarked for suicide prevention. Third, commercial and public health insurers are steadily broadening coverage for behavioral health services, reducing financial barriers to care and increasing the volume of clients seeking help.
Career Ladder: From Hotline to Leadership
A typical progression begins with an entry-level crisis line counselor role, often available to bachelor's-level candidates with crisis intervention training. After earning a master's degree and clinical licensure (LPC, LCSW, or LMFT), counselors transition to licensed clinician positions in hospitals, community mental health centers, or private practice, where they provide direct suicide assessment and safety planning. From there, experienced clinicians move into clinical supervisor roles, overseeing teams of counselors and ensuring adherence to evidence-based protocols. The next rung is program director or clinical director, where responsibilities shift to strategic planning, budget management, and policy development.
For those drawn to research and theory, the academic track offers a parallel path. Pursuing a PhD or PsyD in clinical psychology or a related discipline opens doors to suicidology research, university teaching, and authorship of clinical guidelines. Organizations such as the American Association of Suicidology and the International Academy for Suicide Research actively recruit scholars who can advance the science of prevention.
Lateral Moves and Specialized Roles
Not every counselor seeks upward mobility. Lateral opportunities abound: suicide prevention specialist positions in county and state public health departments focus on community assessment, coalition building, and data surveillance. Training and curriculum development roles at crisis centers design onboarding programs and continuing education modules. Policy and advocacy positions at national organizations like the American Foundation for Suicide Prevention or the Suicide Prevention Resource Center allow clinicians to shape legislation, secure funding, and influence systems-level change. These varied paths illustrate how broad the landscape of counseling careers truly is, with each route leveraging clinical expertise while broadening impact beyond the counseling room.
Frequently Asked Questions About Becoming a Suicide Counselor
Below are answers to the most common questions prospective suicide counselors ask. Each response draws on current licensure standards, employer expectations, and national wage data to help you plan your path with confidence.