

What you’ll learn in this article…
- Child counselors earn a Clinical Mental Health Counseling master's and complete 2,000 to 4,000 supervised clinical hours for licensure.
- School counselors hold state certification rather than clinical licensure and cannot diagnose mental health disorders.
- BLS projects 18% job growth for mental health counselors through 2032, outpacing the 5% rate for school counselors.
- Collaboration between both specialties produces stronger student outcomes when ethical boundaries and referral protocols stay clear.
Both school counselors and child counselors share a core purpose: helping young people thrive. The fork between them, though, is significant. One path centers on developmental guidance inside a K-12 building, covering academic planning, social-emotional learning, and crisis response for entire student populations. The other leads to clinical mental health treatment, diagnosing and treating conditions like anxiety, trauma, and behavioral disorders in children and adolescents across private practices, hospitals, and community agencies.
If you are a prospective graduate student trying to choose between these specialties, the decision turns on more than personal interest. Credentialing timelines, supervised hour requirements, scope of practice restrictions, and salary trajectories all differ in ways that matter long before you see your first client or student.
What Is a Child/pediatric Counselor?
A child or pediatric counselor is a licensed mental health professional who holds a master's or doctoral degree and specializes in assessing, diagnosing, and treating mental health conditions in children and adolescents, typically ages 3 through 18.1 Most child counselors are licensed professional counselors (LPCs) or licensed mental health counselors (LMHCs) who have completed extensive graduate coursework, often 60 or more credits, and supervised clinical hours focused on child and adolescent populations.2 Unlike general therapists who may work with all ages, child counselors receive specialized training in developmentally appropriate interventions and maintain clinical authority to create treatment plans, diagnose disorders according to the DSM, and provide targeted therapy for conditions such as anxiety, depression, trauma, grief, behavioral disorders, and family-related stress.3
Clinical Scope and Treatment Modalities
Child counselors use modalities adapted to developmental stages and cognitive capacities. Play therapy, art therapy, sandtray work, and trauma-focused cognitive-behavioral therapy (TF-CBT) are common tools in their practice.4 These approaches engage children through age-appropriate media rather than relying solely on verbal processing. Family-systems frameworks are also central; child counselors frequently involve parents and caregivers in treatment, recognizing that a child's environment profoundly shapes mental health outcomes. While counselors can administer many clinical assessments and inventories, they are restricted from certain types of psychological testing, specifically, individually administered IQ tests, neuropsychological batteries, and projective personality instruments, which remain within the scope of licensed psychologists.5
Where Child Counselors Work
Child counselors practice in diverse settings beyond school campuses. You will find them in private practices, community mental health centers, pediatric hospitals, outpatient behavioral health clinics, and residential treatment facilities. Some work in collaborative care models within pediatric primary care offices, addressing mental health concerns as part of integrated health services. This breadth of employment options distinguishes child counselors from school counselors, whose roles are tied to educational institutions and often emphasize academic and career guidance alongside social-emotional support.
Child Counselor vs. Child Psychologist: Key Distinctions
A common source of confusion is the difference between a child counselor and a child psychologist. Both specialize in young populations, but their training models and scopes of practice diverge. Child counselors typically hold a master's degree in clinical mental health counseling or a related field and complete a counseling training model focused on wellness, development, and therapeutic relationships.2 Child psychologists earn doctoral degrees (PhD or PsyD) in clinical or school psychology and are trained in psychological assessment, testing, and research design. Psychologists have independent authority to administer and interpret intelligence tests, neuropsychological evaluations, and personality assessments that counselors cannot perform.5 However, in day-to-day clinical therapy (building rapport, conducting intake assessments, diagnosing anxiety or mood disorders, and delivering evidence-based treatment) the roles overlap substantially, and both professionals are qualified to provide high-quality care. Neither child counselors nor child psychologists hold prescription authority; medication management remains the province of psychiatrists and psychiatric nurse practitioners.7
School Counselor Vs. Child Counselor: Side-By-Side Comparison
How do school counselors and child counselors actually differ in salary, job growth, and daily work settings?
Both specialties serve young people, but the distinctions in scope, employment outlook, and credentialing shape very different career trajectories. Here is a direct comparison drawing on federal labor data, professional association standards, and current job market trends.
Salary and Job Growth
The Bureau of Labor Statistics tracks school and career counselors as a distinct occupational category. As of May 2024, the national median annual wage for school and career counselors was $61,710, with projected employment growth of 4% through 2033. Child and pediatric counselors, by contrast, fall under the broader "Substance Abuse, Behavioral Disorder, and Mental Health Counselors" category, which reports a national median wage of $53,710 and notably stronger projected growth of 19% through 2033.
These figures reveal an important tradeoff: school counseling offers a higher median salary and more predictable scheduling tied to academic calendars, while child counseling positions in clinical and community settings show faster job growth reflecting rising demand for youth mental health services.
Work Settings and Caseloads
School counselors are employed almost exclusively in K-12 public and private schools. The American School Counselor Association recommends a student-to-counselor ratio of 250:1, though national averages often exceed 400:1 in underfunded districts. Their scope includes academic planning, career exploration, social-emotional learning, and crisis response within the school day.
Child counselors, sometimes called pediatric counselors, work in private practices, community mental health centers, hospitals, and residential treatment facilities. Caseloads vary widely but typically involve more intensive, one-on-one therapeutic intervention for issues like anxiety disorders, trauma, behavioral challenges, and family conflict. Sessions may extend into evenings or weekends to accommodate families. Students interested in the developmental science behind this work may want to explore child psychology masters programs as a complementary credential path.
Credentialing Differences
School counselors hold state-issued school counseling credentials or certifications, typically requiring a master's degree in school counseling and supervised practicum hours within school settings. The American School Counselor Association offers the Registered Professional School Counselor (RPSC) credential as a supplementary mark of competence.
Child counselors pursue clinical licensure as Licensed Professional Counselors (LPC), Licensed Clinical Professional Counselors (LCPC), or Licensed Mental Health Counselors (LMHC), depending on the state. The Association for Child and Adolescent Counseling, a division of the American Counseling Association, provides specialized training resources and professional development for this population focus.
Employer Expectations
Job postings on major employment platforms reveal distinct skill emphases. School counselor listings prioritize knowledge of educational law, college admissions processes, and group facilitation within classroom settings. Child counselor postings emphasize clinical assessment, evidence-based therapeutic modalities (such as play therapy or cognitive-behavioral therapy for children), and experience with diagnostic criteria.
Both roles require strong rapport-building skills with young clients and their families, but the clinical depth expected of child counselors is typically greater, reflecting their role in treating diagnosable mental health conditions rather than providing developmental guidance.
Questions to Ask Yourself
Education, Licensure, and Certification Requirements
Getting into either specialty starts with graduate-level training, but the specific degree track, clinical requirements, and credentialing pathway differ in ways that will shape your career from day one.
Graduate Program Tracks
Both school counseling and child or clinical mental health counseling programs are typically offered through CACREP-accredited universities, which matters because many state licensing boards and school districts look for that accreditation when evaluating candidates. Exploring available counseling degrees early can help you identify programs aligned with your target specialty.
The two major tracks break down like this:
- School Counseling: Generally 48 to 60 credits, with practicum and internship hours completed in K-12 school settings.1 CACREP standards require at least 100 practicum hours and 600 internship hours, and most programs weave in coursework on career development, college advising, and school-based crisis intervention.2
- Clinical Mental Health Counseling: Typically a 60-credit program, with clinical practicum hours completed in community mental health, private practice, or hospital-based settings.1 The curriculum goes deeper into diagnostic frameworks, treatment planning, and evidence-based therapy modalities used in outpatient work with children and families.
If you plan to work as a child or pediatric counselor in a clinical setting, the Clinical Mental Health Counseling track is the standard route.
Licensure for Child Counselors: LPC and LMHC
After completing your master's degree, becoming a licensed professional counselor requires accumulating supervised post-degree clinical hours. Nationally, that range spans roughly 2,000 to 4,000 hours depending on your state, which is a meaningful difference when you are mapping out your timeline.3
A few state-specific examples illustrate how much variation exists:
- Florida LMHC: 1,500 supervised hours, completed over at least two years4
- Colorado LPC: 2,000 supervised hours3
- California LPCC: 3,000 hours accumulated over a minimum of 104 weeks5
- Connecticut LPC: 3,000 supervised hours and at least 100 hours of direct supervision over two years6
- Massachusetts LMHC: 3,360 total hours, including at least 960 direct client contact hours and 130 supervision hours, completed over two to eight years
Checking your specific state licensing board early is essential because these thresholds directly affect when you can practice independently.
Specialty Credentials for Child-Focused Practice
Licensure gets you in the door, but specialty credentials signal expertise to employers and families seeking child-focused care.
Two credentials worth knowing:
- Registered Play Therapist (RPT): Issued by the Association for Play Therapy, this credential requires a master's degree, licensure, specific coursework in play therapy, and supervised play therapy hours. It is the most recognized marker of advanced training in child-specific therapeutic techniques.
- National Certified Counselor (NCC): Awarded by the National Board for Certified Counselors, the NCC requires passing the National Counselor Examination (NCE) or the National Clinical Mental Health Counseling Examination (NCMHCE).6 It is widely respected across settings and complements state licensure.
School Counselor Credentialing
School counselors follow a different pathway after earning their master's degree. Rather than pursuing clinical licensure, they apply for a state-issued school counseling endorsement or certification through their state's department of education. Requirements vary considerably by state. Some states require a prior teaching certificate or a minimum number of classroom teaching hours. Others substitute the Praxis School Counselor exam or a state-specific competency assessment.
Because school counselor certification is handled at the state education agency level rather than through a health licensing board, candidates moving across state lines often need to re-verify or reapply for credentials even if their degree is from a CACREP-accredited program. Researching your target state's specific requirements before enrolling in a program can save considerable time and cost later.
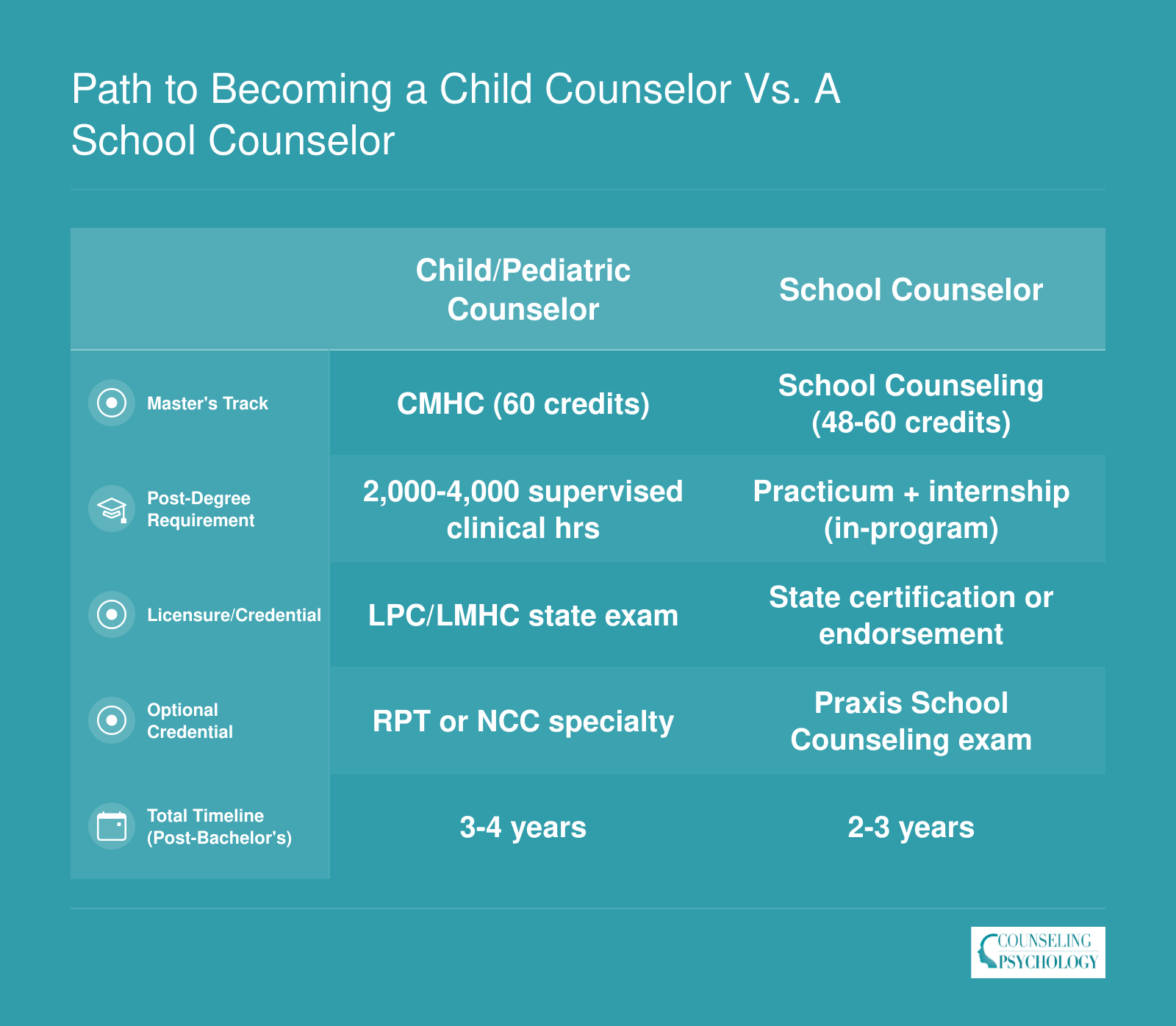
Path to Becoming a Child Counselor Vs. A School Counselor
Both specialties require a bachelor's degree followed by a master's, but the graduate programs, credentialing exams, and post-degree timelines diverge sharply. Child/pediatric counselors typically pursue a Clinical Mental Health Counseling (CMHC) track and spend additional time accumulating supervised clinical hours, while school counselors follow a more structured practicum-to-certification pipeline.
Salary and Job Outlook: School Counselors Vs. Child Counselors
Compensation and demand differ meaningfully between these two paths. School counselors fall under the BLS category Educational, Guidance, and Career Counselors and Advisors (SOC 21-1012), while child and pediatric counselors are captured within Substance Abuse, Behavioral Disorder, and Mental Health Counselors (SOC 21-1018). The mental health counselor category covers a broader population than child specialists alone, so individual salaries may vary depending on setting, caseload focus, and geographic location. Both fields offer solid long-term prospects, though mental health counseling is projected to grow significantly faster over the next decade.
| Metric | School Counselors (SOC 21-1012) | Mental Health Counselors (SOC 21-1018) |
|---|---|---|
| National Median Salary | $65,140 | $59,190 |
| National Mean Salary | $71,520 | $65,100 |
| 25th Percentile Salary | $51,690 | $47,170 |
| 75th Percentile Salary | $83,490 | $76,230 |
| Total Employment (2024) | 376,300 | 440,380 |
| Projected Job Growth Rate (2024 to 2034) | 4% | 19% to 20% |
| Projected Net New Jobs (2024 to 2034) | 13,300 | N/A |
| Estimated Annual Openings (2024 to 2034) | 31,000 | 48,300 |
Related Articles
Highest-Paying States for School Counselors and Mental Health Counselors
Geography plays a significant role in counselor compensation. The tables below show the top-paying states for each occupation category tracked by the BLS. Keep in mind that higher salaries often accompany a higher cost of living, so weigh these figures against local expenses before choosing where to practice.
| State | School Counselor Median Salary | Mental Health Counselor Median Salary |
|---|---|---|
| California | $94,320 | $61,310 |
| Washington | $83,930 | $64,220 |
| District of Columbia | $80,280 | $66,140 |
| Alaska | $80,020 | $79,220 |
| Massachusetts | $78,840 | $59,030 |
| New Jersey | $77,940 | $64,710 |
| New Mexico | $76,490 | $70,770 |
| Oregon | $74,000 | $69,660 |
| New York | $69,900 | $62,070 |
| Connecticut | $70,400 | $62,960 |
| Nebraska | $66,650 | $64,410 |
| Colorado | $63,900 | $59,190 |
| Texas | $65,660 | $60,630 |
| Nevada | $64,960 | $59,470 |
| Wisconsin | $63,690 | $62,470 |
| Wyoming | $65,070 | $61,640 |
Day-To-Day Responsibilities and Child-Specific Interventions
The structured, bell-driven schedule of a school building stands in sharp contrast to the clinical therapy hour, and this distinction shapes every aspect of a counselor's daily routine.
A Day in the Life of a School Counselor
School counselors operate within a multitiered support system that serves all students. Mornings might start with a classroom lesson on emotion regulation or bullying prevention. Midday brings individual check-ins with students struggling academically or socially, followed by small-group sessions on grief or friendship skills. Afternoons often involve collaborating with teachers on student behavior plans, coordinating 504 accommodations, or responding to a crisis.
The American School Counselor Association (ASCA) National Model recommends that at least 80% of a school counselor's time be devoted to direct and indirect student services, with no more than 20% spent on program planning and administrative tasks. In practice, adherence varies widely by district, and counselors frequently juggle duties like test coordination or lunch supervision. For detailed position statements and implementation guides, visit the official ASCA website at schoolcounselor.org. Those interested in advancing further may also explore an online doctorate in school counseling.
A Day in the Life of a Child/Pediatric Counselor
Child and pediatric counselors work in clinics, hospitals, or private practices, delivering focused therapeutic interventions. Each day involves a caseload of individual, family, or group therapy sessions, typically 45 to 50 minutes long. The counselor completes intake assessments, develops treatment plans, and writes progress notes. Sessions rarely look like traditional talk therapy; instead, they incorporate play, art, or sand tray activities to help children express emotions and process experiences.
This role demands extensive clinical documentation and often collaboration with pediatricians, psychiatrists, and child protective services. The pace is deliberately slower than a school setting, allowing for deep, relationship-based work over weeks or months.
Evidence-Based Interventions for Children
Child counselors rely on a range of evidence-based modalities, each suited to specific concerns and age groups:
- Trauma-Focused Cognitive Behavioral Therapy (TF-CBT): Treats trauma symptoms in children aged 3, 18. It combines cognitive-behavioral techniques with trauma-sensitive approaches and is widely researched.
- Parent-Child Interaction Therapy (PCIT): Designed for disruptive behavior disorders in ages 2, 7, PCIT coaches parents in real time to improve the caregiver-child relationship.
- Child-Centered Play Therapy: Grounded in humanistic principles, this approach allows children aged 3, 12 to lead the session through play, fostering self-direction and emotional healing.
- Sand Tray Therapy: A projective technique for all ages, where clients create scenes in a tray of sand, facilitating nonverbal expression and insight.
School counselors trained in these modalities may adapt them for small groups, but clinical child counselors typically use them in intensive, individualized formats. Professionals who focus specifically on childhood trauma counseling often pursue additional certification in TF-CBT or play therapy. The National Child Traumatic Stress Network (nctsn.org) and the Association for Play Therapy (a4pt.org) provide treatment summaries, age ranges, and research bibliographies for these and other interventions.
Time Allocation and Job Outlook
The U.S. Bureau of Labor Statistics offers employment projections for school and mental health counselors, but time-allocation data often comes from surveys and district reports. Because the ASCA 80/20 rule is a recommendation rather than a mandate, prospective school counselors should investigate local practices by reviewing state department of education websites or recent job postings. For child counselors, productivity expectations vary by employer; community mental health settings may require a higher number of weekly direct-service hours than private practice. Checking BLS.gov for current outlook figures and then verifying with state-specific resources will give you the most realistic picture.
School counselors cannot diagnose mental health disorders. They are trained to screen for concerns and identify warning signs, but diagnostic authority rests with licensed clinical counselors (LPC, LMHC) or psychologists. When a student presents symptoms of anxiety, depression, or other conditions, school counselors refer to external clinicians who hold the scope of practice to assess and diagnose under state law.
How School Counselors and Child Counselors Collaborate
Effective collaboration between school counselors and community-based child counselors hinges on clear ethical boundaries, shared protocols, and mutual respect for each discipline's scope. When these two professionals coordinate care, students receive more comprehensive support, but only if both parties navigate privacy regulations, referral standards, and communication frameworks with precision.
Referral Protocols and Ethical Foundations
Both professions operate under distinct ethical codes that govern inter-professional collaboration. School counselors follow the ASCA Ethical Standards for School Counselors, which outline referral procedures, parental consent requirements, and the duty to coordinate with outside providers when a student's needs exceed the scope of school-based services. The American Counseling Association's Code of Ethics, particularly Section D (Relationships With Other Professionals), provides detailed guidance on how licensed child counselors should communicate with educators, maintain client autonomy, and respect boundaries when working alongside school personnel. These documents are freely available on the ASCA and ACA websites and serve as the foundational texts for defining roles, consent processes, and confidentiality obligations.
FERPA, HIPAA, and Information Sharing
One of the most complex facets of collaboration involves reconciling two privacy frameworks. School counselors operate under the Family Educational Rights and Privacy Act (FERPA), which protects education records and allows parents broad access to their child's school files. Licensed child counselors in private practice, clinics, or hospitals are bound by the Health Insurance Portability and Accountability Act (HIPAA), which imposes stricter confidentiality protections and limits disclosure without explicit written consent. The U.S. Department of Education publishes FERPA guidelines, and the Department of Health and Human Services offers HIPAA FAQs for mental health providers; both resources clarify when records may be shared and when separate consent is required. Always cross-reference these federal regulations with local school district policies, which may impose additional consent or documentation requirements.
Coordination Models and Partnership Frameworks
Successful collaboration typically follows one of several evidence-based models. ASCA publishes position statements on collaboration and school-community partnerships that outline tiered support systems, case-consultation protocols, and shared-care agreements. The Substance Abuse and Mental Health Services Administration (SAMHSA) website offers additional frameworks for integrating behavioral health services into educational settings, including memoranda of understanding templates and data-sharing agreements. Real-world examples of these partnerships can be found in state school counselor association conference proceedings and on community mental health agency websites that publish case studies demonstrating how referral pathways, joint treatment planning, and outcome monitoring work in practice.
Practical Collaboration in Action
In day-to-day practice, collaboration often begins with a warm handoff: the school counselor identifies a student in need of clinical intervention, secures parental consent, and provides the external counselor with relevant context (academic concerns, behavioral observations, social stressors). The child counselor then conducts a full assessment, develops a treatment plan, and periodically updates the school counselor (with guardian permission) on progress and any accommodations that might support the student's functioning in the classroom. In cases involving trauma histories, a specialist trained in childhood trauma counseling may join the care team to address needs that require targeted clinical expertise. Both professionals respect each other's expertise: the school counselor focuses on academic and social development within the educational environment, while the licensed child counselor addresses clinical diagnoses, trauma processing, and therapeutic interventions that fall outside the school counselor's training and role.
Choosing Your Specialty: Key Decision Factors
Neither path is universally better; the right choice depends on how you want to spend your working hours and whom you want to serve. Weigh these practical trade-offs before committing to a degree track or certification route.
Pros
- School counselors benefit from a predictable academic calendar, including summers off in many districts, which supports work-life balance.
- School counseling positions typically offer state employee benefits such as pension plans, health insurance, and tuition reimbursement.
- Child and pediatric counselors enjoy deeper clinical autonomy, choosing therapeutic modalities and tailoring treatment plans for each young client.
- Private practice as a child counselor allows flexible scheduling and the potential for higher per-session earnings once a caseload is established.
- School counselors reach large numbers of students through group programming, making prevention-focused work possible at a community scale.
- Child counselors can specialize in niche areas like trauma, play therapy, or neurodevelopmental disorders, building highly marketable expertise.
Cons
- School counselors often carry caseloads well above the recommended 250:1 ratio, limiting time for individual student support.
- Child counselors in private practice face unpredictable income early on, along with the overhead costs of running a business.
- School counselors may spend significant time on administrative duties like scheduling and testing coordination rather than direct counseling.
- Licensure as a clinical child counselor requires thousands of supervised post-graduate hours, delaying full independent practice by two or more years.
- School counselor roles are tied to district budgets, so positions can be cut during funding shortfalls despite student need.
- Child counselors working with severe cases, such as abuse or suicidal ideation in minors, face elevated risks of compassion fatigue and burnout.
Frequently Asked Questions
These are among the most common questions students ask when weighing a school counseling path against a child or pediatric counseling specialty. The answers below draw on current credential standards, BLS wage data, and widely recognized professional frameworks.







