What you’ll learn in this article…
- Black professionals make up 4% of psychologists and 2% of psychiatrists in the United States.
- Dr. Cheyenne Bryant’s credentials sparked an online debate over therapist licensure versus coaching.
- Historical medical abuse makes credential distrust a rational protective response in Black communities.
In May 2026, a viral debate over Dr. Cheyenne Bryant's credentials thrust a long-simmering question into public view: when Black communities seek mental health support, how do they know who is truly qualified? For counselors, the moment exposed a pressing need to confront distrust that is rooted in history and sustained by stark underrepresentation. According to the Association of Black Psychologists, only 4% of psychologists and 2% of psychiatrists in the U.S. are Black.1
That gap fuels a difficult calculus for Black clients, who may weigh licensed clinicians against unregulated coaches and influencers offering cultural familiarity without diagnostic training. The choice is not merely personal; it reflects systemic failures that demand a transparent response from the field. Building trust means acknowledging why credentials alone do not reassure, and proving, through clinically sound and culturally responsive care, that licensure protects rather than excludes.
The Online Debate Over Mental Health Credentials: What Happened and Why It Matters
What Sparked the Debate
In spring 2026, social media platforms lit up with questions about the professional standing of Dr. Cheyenne Bryant, a prominent psychology personality whose advice and background suddenly faced intense public scrutiny. Writing for Ebony on May 27, 2026, journalist Tamieka Welsh traced how an online exchange quickly became a flashpoint for a broader reckoning.1 What began as individual skepticism about one person's credentials mushroomed into a cultural interrogation of who gets to speak with authority on mental health in Black communities. The central friction is this: audiences often feel a powerful sense of recognition and cultural safety when a figure shares their lived experience, but relatability alone does not guarantee clinical competence, ethical training, or any form of regulatory accountability.
Credentialed Clinicians vs. Coaches vs. Influencers
Licensed clinical marriage and family therapist Jordan A. Madison, founder of Therapy is My JAM, offered a crucial distinction in the same article. Licensed mental health professionals, whether LCSWs, therapists, psychologists, or psychiatrists, operate under clear state mandates. They complete supervised clinical hours, pass rigorous national exams, undergo background checks, and earn continuing education credits for psychologists every two years to keep their licenses active.1 Life coaches, by contrast, are not licensed in any jurisdiction; they focus on personal development, future goals, and accountability, not on diagnosing or treating mental health conditions. Influencers speak from personal experience, building trust through authenticity and relatability, but they carry none of the formal oversight or ethical enforcement that protects clients. These are distinct roles, yet the public discourse frequently blurs them, particularly when a trusted voice delivers mental health content.
Why This Debate Demands Professional Attention
For practitioners in forensic and clinical psychology, counseling, social work, and marriage and family therapy, this is not a transient social media spat. It exposes a genuine crisis of confidence in credentialed care among Black Americans, with real stakes for public safety and professional integrity. Data from the Association of Black Psychologists underscores the problem: only 4% of psychologists, 2% of psychiatrists, and 7% of marriage and family counselors in the U.S. are Black.1 As our reporting on BIPOC therapists in the U.S. details, this underrepresentation fuels the very skepticism communities express online. When communities have historically endured exclusion, misdiagnosis, and maltreatment within health systems, it is entirely reasonable that cultural resonance and shared identity may seem more trustworthy than a license. But that same history places a heightened duty on licensed professionals. Clinicians must be ready to articulate what licensure means, why it protects the public, and how it coexists with cultural humility, not as a defensive posture, but as a core ethical obligation to the communities they serve.
Licensed Therapist Vs. Life Coach Vs. Influencer: What Black Communities Need to Know
The rapid growth of mental health content on social media has blurred the lines between licensed clinical care and personal advice, sparking crucial conversations in Black communities about who is truly qualified to treat mental illness. As Jordan A. Madison, a licensed clinical marriage and family therapist, explained to Ebony, licensed therapists must adhere to state boards, rules, regulations, background checks, and complete continuing education credits every two years, a level of accountability that coaches and influencers do not share.1
The Core Differences in Training and Oversight
Licensed mental health professionals operate under strict regulatory frameworks that ensure public safety. Each credential reflects a distinct educational pathway in counseling vs psychology vs social work, supervised clinical experience, and an examination process:
- Licensed Clinical Social Worker (LCSW): Requires a Master's in Social Work, approximately 3,000 hours of supervised clinical experience, and passing the ASWB Clinical Exam. They assess, diagnose, and treat mental and behavioral disorders.
- Licensed Professional Counselor (LPC): Holds a Master's in Counseling, completes 2,000 to 3,000 clinical hours, and passes the NCE or NCMHCE. Their scope includes diagnosing and treating mental disorders through psychotherapy.3
- Licensed Marriage and Family Therapist (LMFT): Earns a Master's in Marriage and Family Therapy, logs 2,000 to 3,000 clinical hours, and passes the AMFTRB National MFT Exam. They specialize in diagnosing and treating disorders within relational and family systems.
- Psychologist: Requires a doctoral degree (PhD, PsyD, or EdD), about 3,500 hours of supervised practice, and passing the EPPP plus state exams. They have broad authority to assess, diagnose, and treat mental illness, including psychological testing.5
- Psychiatrist: As medical doctors (MD or DO), they complete a four-year psychiatric residency, pass the USMLE or COMLEX, and earn board certification. They can prescribe medication and manage complex biological aspects of mental health.
All licensed professionals must fulfill ongoing continuing education requirements, typically 30 to 40 hours every two years, and are subject to state board oversight, which can discipline or revoke licenses for ethical violations.
Life Coaches and Influencers: Where Credentials Stop
Life coaches operate without legal licensure. No specific degree is mandated, no clinical hours are required, and no board evaluates their competence. Their role is limited to goal-setting and personal development; they cannot diagnose or treat mental disorders. As Madison noted, coaching focuses on future aspirations, not clinical healing.1 Mental health influencers, meanwhile, often draw on lived experience alone. While their stories can destigmatize seeking help, their advice is not grounded in clinical training, diagnostic frameworks, or ethical codes. Understanding the difference between licensure and non-licensure pathways is essential for consumers evaluating a provider's qualifications.
Why the Distinction Matters for Black Mental Health
For Black clients navigating a system historically marred by mistrust, the line between licensed care and unregulated advice carries high stakes. Misunderstanding these distinctions can lead someone with a treatable condition, such as depression or trauma, to receive coaching that fails to address underlying pathology, or to follow influencer guidance that inadvertently causes harm. Licensed professionals are trained to recognize cultural contexts while adhering to scientific standards; unlicensed practitioners are not held to any such obligation. Knowing the difference empowers Black communities to seek care that is both culturally attuned and clinically rigorous.
Questions to Ask Yourself
Why Black Americans Distrust the Mental Health System: Historical and Structural Roots
Credential skepticism does not emerge in a vacuum. For many Black Americans, distrust of the mental health system is a legacy of institutional betrayal that continues to shape how licenses, degrees, and board certifications are perceived.
A Legacy of Harm: From Enslavement to the 20th Century
The roots run deep. In the 19th century, Dr. J. Marion Sims performed experimental surgeries on enslaved Black women without anesthesia, cementing a medical culture that dehumanized Black bodies. The infamous Tuskegee syphilis study, spanning four decades, deliberately withheld treatment from Black men under the guise of research, eroding trust in public health institutions for generations. This history extended into mental health: during the civil rights era, Black activists were disproportionately diagnosed with schizophrenia, a label weaponized to pathologize resistance and justify institutionalization.
Modern Mistrust in Numbers
These events are not distant memories. Pew Research Center surveys consistently show that Black Americans report lower trust in medical and mental health institutions compared to white Americans. A 2024 Pew report found that only 53% of Black adults expressed confidence in medical scientists to act in the public's interest, compared to 68% of white adults.1 When institutions have been responsible for harm, skepticism toward their gatekeeping mechanisms, like licensure boards, becomes a protective instinct rather than ignorance. The persistent mental health workforce shortage compounds the problem, leaving many Black communities without adequate access to credentialed providers who understand their lived experience.
Skepticism as Rational Self-Protection
Credentialism alone cannot overcome a history of abuse. Licenses signal adherence to standards, but those standards were historically used to exclude or pathologize Black people. The mental health system still struggles with cultural competence, misdiagnosis, and implicit bias. For Black clients, questioning a provider's credentials is not a rejection of expertise; it is a demand for accountability. Students exploring careers in this field should consider how resources like the mental health education guide for Black students can prepare them to practice with the cultural humility these communities require. Trust must be earned through demonstrated ethical practice, not assumed from a diploma on the wall.
Intersecting Identities Shape Distrust
Distrust is not monolithic. Age, gender, LGBTQ+ identity, and immigration status all influence how skepticism manifests. Black LGBTQ+ individuals may face compounded mistrust after histories of conversion therapy, while Black immigrants navigate cultural stigmas layered on systemic ones. Counselors must recognize that each client's relationship with the mental health system is shaped by multiple, intersecting histories of marginalization.
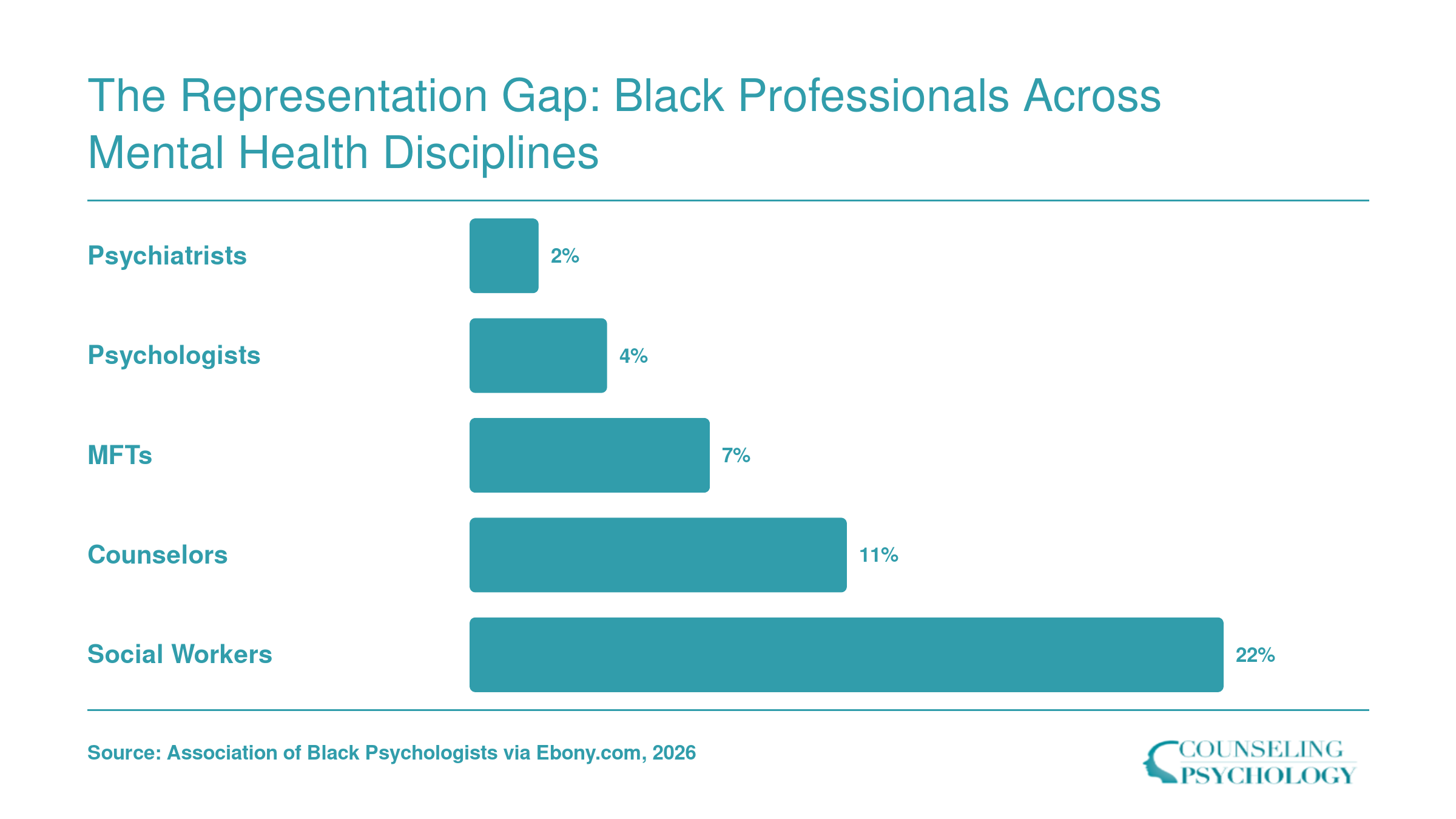
The Representation Gap: Black Professionals Across Mental Health Disciplines
Does Racial Concordance in Therapy Actually Improve Outcomes?
Racial concordance can strengthen the therapeutic alliance and keep Black clients in treatment longer, but it is neither a magic bullet nor a substitute for genuine cultural competence.
The Evidence on Retention and Early Dropout
A robust psychotherapy meta-analysis examining ethnic minority clients, including Black participants, found that racial/ethnic matching modestly reduces premature termination, with an effect size of 0.2, 0.3 and an odds ratio of 0.7, 0.8.1 In practical terms, Black clients working with a Black therapist are roughly 20, 30% less likely to drop out of therapy early compared to those with non-Black therapists. Retention is a critical gatekeeper to progress, because clients who stay engaged receive a larger dose of treatment. However, that same body of research showed symptom reduction effects near zero, meaning that race matching alone did not translate into measurably better clinical outcomes.1
Beyond Dropout: What the Data Show About Satisfaction and Communication
Broader healthcare concordance literature adds texture. A 2025 review of patient-provider race matching found consistently higher patient satisfaction, improved communication quality, and greater participatory decision-making when clinicians and clients share a racial background.2 In the addiction treatment space, a 2024 scoping review of 11 studies focused exclusively on Black patients reported that concordance was not associated with treatment access or formal engagement measures, but it did increase perceived empathy.1 Together, these findings suggest that racial concordance may improve relational factors, including client comfort, perceived understanding, and the sense of being heard, without automatically changing depression scores or anxiety levels.
The Missing Piece: Cultural Competence and Humility
Caution is essential when interpreting concordance effects. A Black therapist who lacks cultural humility training may still default to colorblind approaches, minimize the impact of racism, or overlook the cultural meaning of distress, eroding trust just as quickly as a non-Black provider. Research consistently shows that therapist multicultural counseling competence, rather than demographic matching alone, predicts therapeutic alliance and client satisfaction. Concordance can open the door, but a therapist's willingness to validate racial experiences, explore identity, and adapt interventions determines whether the client walks through it.
The Representation Gap Limits Concordance as a Standalone Solution
With Black psychologists and psychiatrists making up just 4% and 2% of their fields respectively, and professional counselors at 11%, simply matching client and therapist by race is logistically impossible for most Black help-seekers. Demand far outstrips supply, and geographic, financial, and scheduling barriers compound the shortage. Even if concordance reliably boosted outcomes, the field cannot scale it to meet need. This reality forces a hard look at alternative strategies: training all clinicians to deliver culturally responsive care, integrating peer support and community health workers, and redesigning service delivery to be genuinely inclusive.
What This Means for the Field
The data support a two-pronged imperative. First, intentional workforce diversification through targeted recruitment, debt relief programs, and retention efforts remains urgent. Second, every training program and licensure pathway must embed rigorous cultural competence curricula, not as an elective but as a core clinical skill. For individual practitioners, the takeaway is clear: racial concordance is a door you may or may not have, but cultural humility is a door you must build yourself. The trust of Black clients depends not on who you are, but on how well you prove you are safe.
Credentials are designed to protect clients, yet the mental health system has historically harmed Black communities. Counselors must hold both truths: validating skepticism while demonstrating accountability, not dismissing distrust as ignorance.
How Distrust Shows up in the Therapy Room, and What Counselors Can Do
Distrust rooted in historical mistreatment and systemic inequities does not vanish when a Black client sits on your couch. It can surface in subtle and overt ways, shaping the therapeutic alliance from the first session. Recognizing these signals and responding with research-informed strategies is central to providing ethical, effective care.
Recognizing the Signs of Cultural Mistrust
Cultural mistrust often appears as guardedness or skepticism that can be mistaken for resistance. Clients may test the therapist's credibility, asking pointed questions about qualifications or experience with Black communities. They might withhold sensitive information, share only surface-level concerns, or disengage when race-related topics arise. Some clients display a hypervigilance to perceived microaggressions, scrutinizing word choice and nonverbal cues. These behaviors are not pathology; they are adaptive self-protective strategies born from generations of harm in healthcare settings. Counselors who interpret such responses as simply "noncompliance" risk deepening the rupture.
The Multicultural Orientation Framework
A growing body of professional guidelines and peer-reviewed research emphasizes the Multicultural Orientation framework. This approach shifts the focus from therapist competence (a checklist of knowledge) to an ongoing, relational process of cultural humility, cultural comfort, and attending to cultural missed opportunities. Cultural humility involves the therapist's willingness to see the client as the expert on their cultural experience and to learn from each interaction. Cultural comfort reflects the therapist's ease in discussing racial dynamics without defensiveness. When missteps occur, the therapist actively repairs by acknowledging the rupture and inviting dialogue. This framework, endorsed in writings by researchers like Hook and colleagues, offers a practical roadmap for turning moments of distrust into opportunities for deeper connection. Counselors interested in building these competencies can explore a structured path through multicultural therapy training programs.
Broaching as a Clinical Technique
One specific evidence-informed intervention is broaching: the therapist's explicit effort to bring cultural factors into the conversation. Research suggests that when therapists initiate discussions about race, ethnicity, and power early in treatment, clients feel more understood and report greater satisfaction. Broaching can be as straightforward as saying: "I want to acknowledge that our identities differ in important ways. How might that affect your comfort in talking with me?" It signals that the therapist is not colorblind, but attuned to the reality that race shapes life experiences. When broaching is missing, clients may perceive the therapist as evasive or uninformed, which can validate pre-existing suspicions. Training resources from organizations like the Association for Multicultural Counseling and Development provide scripts and practice guidelines to help counselors develop this skill.
Practical Steps for Counselors
Building trust with Black clients requires deliberate, ongoing effort. Start by consulting the ethics codes and practice resources published by the American Counseling Association and the American Psychological Association; both offer free articles and webinars on multicultural orientation. Seek continuing education through the National Board for Certified Counselors or similar bodies that address cultural mistrust and humility. In session, normalize feedback: explicitly invite clients to share if something felt off or if a comment landed poorly. Consider environmental cues. Are your waiting room materials and decor inclusive? Do your intake forms ask about strengths and cultural background rather than assuming a deficit lens? Scheduling regular peer consultation focused on cultural dynamics can also reduce isolation and blind spots.
Ultimately, the goal is not to erase mistrust but to earn a relational credibility that allows clients to engage safely. When counselors demonstrate consistency, humility, and a genuine commitment to understanding, they disrupt the narrative that mental health care is not for Black communities. This work is challenging, but it sits at the heart of ethical practice.
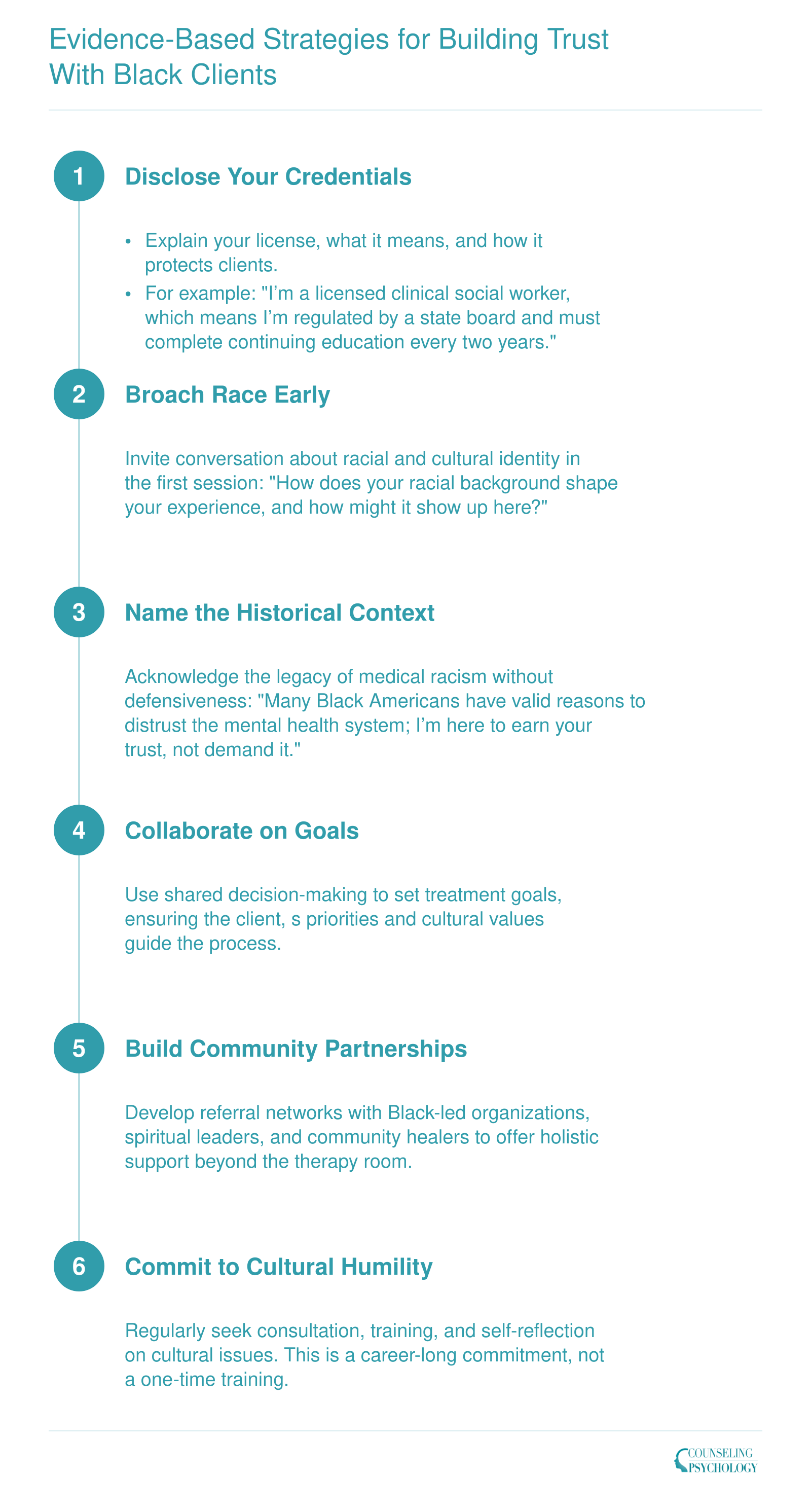
Evidence-Based Strategies for Building Trust With Black Clients
Building trust with Black clients is not a one-time gesture but a sustained clinical practice. The following framework offers actionable steps counselors can integrate from intake through ongoing treatment, each grounded in cultural humility and transparency.
Community-Based Alternatives and Collaborative Care Models
As trust in conventional mental health systems remains fragile in Black communities, more counselors and agencies are exploring community-based models that prioritize cultural relevance and accessibility. These programs are not designed to replace licensed clinical care, but they offer promising alternatives for prevention, early intervention, and support for people who might otherwise never engage with the mental health system.
The Rise of Community-Driven Mental Health Support
Community-anchored initiatives have emerged over the past decade as a direct response to longstanding barriers: stigma, cost, lack of culturally attuned providers, and a deep-seated skepticism rooted in historical mistreatment. By embedding mental health support in familiar settings (barbershops, churches, salons, and neighborhood centers), these programs reduce the psychological distance between a person in distress and a helping conversation.
One frequently cited example is The Confess Project, a barbershop-based mental health initiative that trains barbers to serve as mental health advocates. Barbers, already trusted figures in many Black communities, learn to listen actively, recognize signs of distress, and bridge clients to professional resources. Similar models partner with pastors and other faith leaders to integrate emotional wellness into church programming, offering everything from psychoeducation workshops to short-term pastoral counseling with clearly defined referral pathways.
Peer support networks also play a growing role. Some are organized around shared identity or lived experience, such as groups for Black fathers, survivors of violence, or LGBTQ+ youth. These networks are often less formal than clinical services but can provide powerful social connection and normalization of help-seeking.
How to Identify Credible Community Programs
For clinicians interested in referring clients or building partnerships, vetting community-based programs requires the same diligence applied to any clinical resource. The following strategies can help counselors evaluate program quality and evidence base:
- Search academic databases: Use PubMed, PsycINFO, or Google Scholar with terms such as "barbershop mental health," "church-based counseling Black," or "Afrocentric therapy effectiveness." Look for peer-reviewed studies that report at least qualitative outcomes.
- Review program websites and reports: Many well-established initiatives publish case studies, white papers, or outcome summaries. For instance, The Confess Project and some federally funded programs share evaluation data. The American Counseling Association (counseling.org) also maintains a resource library that occasionally features such models.
- Explore foundation and government resources: The Substance Abuse and Mental Health Services Administration (SAMHSA) and the Robert Wood Johnson Foundation have funded and evaluated culturally tailored interventions. Their websites often include implementation guides and programmatic outcome reports.
- Connect with university research centers: Schools of public health at institutions like Johns Hopkins or the University of Michigan have produced research on faith-integrated and community-based interventions. Faculty may be able to direct you to working papers or community partnerships that are not yet widely published.
Collaborative Approaches for Licensed Professionals
When community models are credible and well-structured, clinicians can collaborate in ways that strengthen both the informal support network and the clinical service continuum. Professionals exploring alternative careers with an MFT degree may find that community partnership roles represent a meaningful extension of their training. Some practical strategies include:
- Co-locating services: Placing a licensed therapist within a church, barbershop, or community center on a rotating schedule can bring clinical expertise directly into a trusted space.
- Referral networks: Establishing clear, warm handoff protocols between community advocates and mental health clinics ensures that people who need higher-level care receive it without falling through the cracks.
- Co-facilitation: Clinicians may co-lead psychoeducational groups with peer supporters, blending professional knowledge with community credibility.
- Cultural consultation: Community advocates and faith leaders can serve as cultural consultants to clinics, helping providers adapt treatment approaches to be more congruent with client worldviews.
Considerations for Cultural Competence and Ethical Practice
While community-based alternatives are valuable, licensed professionals must remain mindful of scope of practice boundaries. Untrained advocates should never be mistaken for diagnosticians or clinicians, and formal referral mechanisms are essential. Counselors also need to examine their own biases: romanticizing community models without critical evaluation can lead to harm. The most effective partnerships occur when both sides respect each other's expertise and limitations, and when the client's well-being remains the primary goal.
Questions Black Clients Can Ask to Evaluate a Therapist's Credentials and Cultural Competence
Asking the right questions before committing to therapy can transform a vulnerable process into an empowered partnership. For Black clients who often navigate systems steeped in historical harm, direct inquiry is not an imposition; it is a safeguard. The following questions, drawn from clinical best practices and the insights of culturally responsive practitioners, serve a dual purpose: they equip clients to assess fit and invite therapists to examine their own preparation.
What to Ask About Credentials
- Licensure: What license do you hold, and which state board oversees your practice? Can you explain the difference between your clinical training and the role of a life coach or influencer?
- Scope of practice: Are you able to diagnose mental health conditions and provide treatment, or do you focus on coaching and personal development?
- Continuing education: How do you stay current? Can you give an example of a recent continuing education course relevant to Black mental health?
- Background and accountability: Do you have a record of any disciplinary actions? How does your licensing board handle complaints?
Assessing Cultural Competence
- Training history: What specific coursework, certifications, or workshops have you completed on working with Black communities? Be as concrete as possible.
- Race and therapy: How do you bring up race in sessions? If a client wanted to talk about racism, discrimination, or microaggressions, how would you respond?
- Lived experience: While therapists are not required to share personal backgrounds, can you describe how you stay informed about issues affecting Black Americans?
- Past challenges: Tell me about a time a cultural misunderstanding occurred with a client. How did you repair it?
Understanding Clinical Approach
- Rupture and repair: How do you handle disagreements or moments of tension in the therapeutic relationship? What does repair look like with you?
- Feedback and supervision: Do you engage in ongoing supervision or peer consultation that focuses specifically on cultural dynamics? How do you incorporate client feedback into treatment?
Red Flags to Notice
Even a skilled clinician may respond poorly when questioned. Watch for defensiveness about credentials, such as vague answers like "I'm certified" without naming a licensing board. Dismissing race with phrases like "I treat everyone the same" or "I don't see color" signals a lack of cultural humility. An inability to name any specific training on Black mental health, or a reluctance to discuss supervision or consultation, suggests a gap in self-reflection. Finally, be cautious of promises of quick fixes or pressure to commit to expensive packages; ethical therapy is collaborative, not transactional.
A Tool for Practitioners
Counselors can proactively share this list during initial consultations or on their websites. Transparency does not replace trust; it accelerates it. When a therapist says, "Here are questions I invite every client to ask," the power dynamic shifts toward partnership. Practitioners looking to deepen their skills in this area may benefit from exploring multicultural therapy training programs and pursuing supervision that centers cultural dynamics. For practitioners, the list also functions as a self-audit: if answering any item feels uncomfortable, that discomfort points to an area for growth. Those who want structured feedback on their LMFT supervision hours and cultural competence obligations can use their state board's requirements as a benchmark. By normalizing credential checks and cultural competence inquiries, the profession moves closer to the safety and equity Black communities deserve.
Frequently Asked Questions
Mental health professionals and students often encounter questions about trust and cultural competence when working with Black communities. Here are clear answers to some of the most common concerns.