What you’ll learn in this article…
- Research shows that most college students who have experienced trauma never connect with campus support services.
- SAMHSA's six core principles, including safety, trustworthiness, and collaboration, provide the framework campuses use to become trauma-informed.
- A realistic campus implementation timeline spans four phases, from needs assessment through sustained evaluation and refinement.
- Careers in trauma-informed campus work range from residence life coordinators to licensed counselors, each requiring distinct credentials.
Nearly every accredited college operates a counseling center staffed by licensed therapists, yet most campuses still design housing policies, classroom protocols, and conduct systems as if trauma were rare or irrelevant. Trauma-informed care means intentionally organizing every campus touchpoint to acknowledge that trauma exposure is common, to avoid retraumatization, and to support recovery and resilience, rather than confining that awareness to clinical offices alone.
The gap between clinical competence and campus-wide practice reflects inertia more than intent. Provosts, residence life directors, and campus safety teams may never have learned the SAMHSA principles that underpin trauma-informed work, and few institutions train faculty in the neurobiology of stress or design flexible absence policies that reduce dropout among students with post-traumatic stress.
This guide walks through prevalence data that justifies the shift, adapts core trauma-informed principles for higher education contexts, maps a phased implementation roadmap, highlights identity-specific considerations for marginalized student populations, and outlines career paths for students interested in building trauma-responsive campus environments after graduation.
How Common Is Trauma Among College Students?
The American College Health Association's National College Health Assessment, which has surveyed more than 2.5 million students across 1,000 institutions through 2024, provides a clearer picture of trauma exposure on campus than ever before.1 While the survey does not replicate the original CDC-Kaiser Adverse Childhood Experiences (ACE) study methodology, its findings on personal safety and violence align with broader national data showing that a substantial proportion of young adults enter college already carrying a trauma history.2 The CDC's ACE framework categorizes childhood adversity across abuse, neglect, and household dysfunction; national surveys consistently find that individuals aged 18 to 25 report ACE exposure at rates comparable to or higher than older cohorts, with estimates suggesting that more than half of young adults have experienced at least one category of adversity before reaching campus.
Sexual Assault and Interpersonal Violence
Campus-specific prevalence data underscores the urgency of trauma-informed approaches. Multiple large-scale surveys indicate that approximately one in five undergraduate women and one in sixteen undergraduate men experience sexual assault during their college years. Interpersonal violence, including dating violence and stalking, affects a significant minority of students across gender identities. The ACHA-NCHA surveys capture self-reported exposure to violence and safety concerns; the Spring 2025 reference group drew on responses from 65,950 students, while the Fall 2024 survey included 30,000 students from 50 institutions.34 These snapshot reports reveal persistent exposure to traumatic events during the college years themselves, layered atop any childhood trauma counseling needs students bring with them.
PTSD and the Utilization Gap
Post-traumatic stress disorder prevalence among 18- to 25-year-olds exceeds that of the general adult population, with published estimates ranging from 8 to 12 percent in this age bracket. Yet only about 35 percent of college students utilized psychological services in Spring 2024, and not all of that utilization addresses trauma specifically. The gap between trauma exposure and formal help-seeking is wide: many students who meet criteria for trauma-related diagnoses never step foot in a campus counseling center, relying instead on informal peer support, avoidance, or silence.
Compounding Risk Factors During the College Transition
The transition to college introduces stressors that can amplify the impact of prior trauma. Students navigate living independently for the first time, exploring identities around sexuality, gender, spirituality, and politics while managing academic demands and often significant financial pressure. For students facing housing insecurity or other basic-needs crises, the challenges are even steeper, as resources like help for homeless students may be difficult to locate. For trauma survivors, these developmental tasks unfold against a backdrop of hypervigilance, emotional dysregulation, or mistrust, raising the stakes for institutions to embed trauma-informed practices across residence life, academic advising, financial aid offices, and every corner of campus where students seek support.
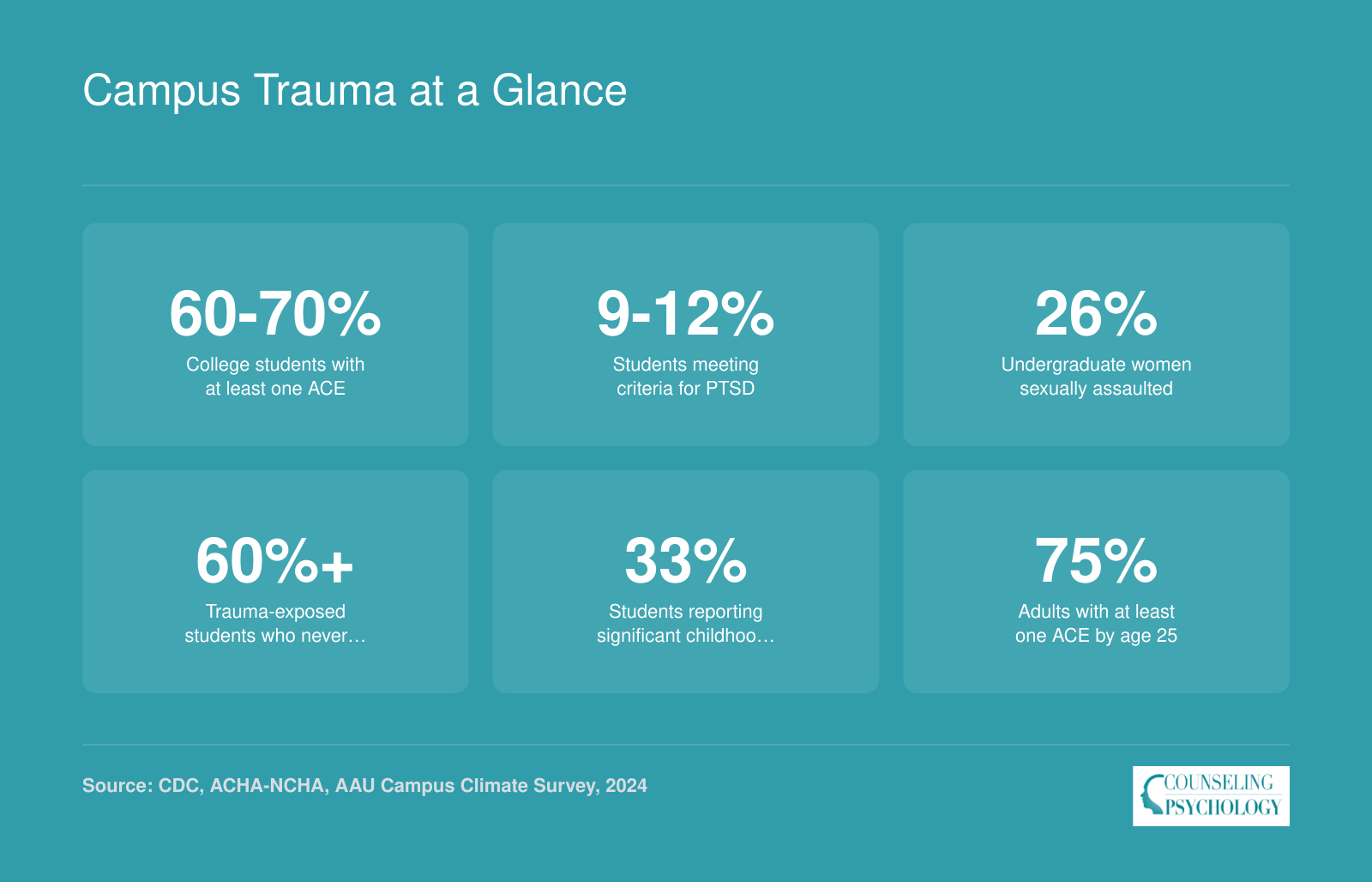
Campus Trauma at a Glance
Trauma exposure among college students is far more common than many administrators realize, and most affected students never connect with campus support services. These figures underscore why embedding trauma-informed practices across every campus touchpoint matters.
Core Principles of Trauma-Informed Care in Higher Education
What does it actually mean for a campus to be trauma-informed, and how is that different from simply having a counseling center?
The distinction matters more than most administrators realize. A university can employ excellent therapists and still operate in ways that re-traumatize students, from rigid attendance policies that punish crisis-related absences to residence-life protocols that strip autonomy during welfare checks. Being trauma-informed is not about adding a single service. It is about redesigning systems, policies, and culture so that every touchpoint on campus reflects an understanding of trauma's impact.
SAMHSA's Six Principles, Applied to Campus Life
The Substance Abuse and Mental Health Services Administration (SAMHSA) identifies six core principles of a trauma-informed approach. Each one translates directly into higher-education practice.
- Safety: Classrooms, residence halls, and common spaces are designed so students feel physically and psychologically secure. A campus example: faculty post content advisories before screening graphic material and offer alternative assignments without penalty.
- Trustworthiness and transparency: Institutional decisions, from disciplinary procedures to tuition changes, are communicated clearly and consistently. Students know what to expect and why.
- Peer support: Trained peer educators and recovery mentors are embedded in orientation, residence life, and student organizations, creating pathways to help that do not require a clinical appointment.
- Collaboration and mutuality: Students participate in governance committees that shape campus mental-health policy, rather than being passive recipients of top-down programming.
- Empowerment, voice, and choice: Advising and student-conduct processes offer meaningful options. A student reporting sexual assault, for instance, can choose between formal investigation and supportive measures without being forced into a single track.
- Cultural, historical, and gender issues: Programming acknowledges that systemic racism, colonialism, heteronormativity, and other structural forces shape how trauma is experienced and disclosed. Counseling intake forms include inclusive language and identity-affirming options.
When these six principles are woven into policy, training, and daily operations, the entire institution becomes the intervention, not just the counseling office.
Trauma-Informed Care Versus Trauma-Specific Treatment
Readers sometimes conflate the organizational framework with clinical therapy. Trauma-informed care is the ecosystem: the attitudes, practices, and policies that create a safe environment campus-wide. Trauma-specific treatment refers to clinical modalities delivered by licensed professionals to individuals diagnosed with PTSD or related conditions. Evidence-based treatments for PTSD, such as Cognitive Processing Therapy (CPT), Prolonged Exposure (PE), and Eye Movement Desensitization and Reprocessing (EMDR), sit inside a trauma-informed system, but they are not the whole system.
Think of it this way: CPT or EMDR is the specialized tool a campus therapist uses in session. Trauma-informed care is the reason the student felt safe enough to walk through the counseling center door in the first place, and the reason their professor did not penalize them for missing class to get there.
Why Siloed Services Fall Short
Campuses that treat trauma response as the counseling center's job alone tend to see the same problems cycle year after year: low utilization rates, long waitlists, and high rates of student attrition among trauma-exposed populations. Professionals trained as crisis intervention specialists play a valuable role, but systemic redesign distributes awareness and responsibility across academic affairs, student life, financial aid, campus safety, and every department that touches a student's daily experience. That shift, from siloed service to shared commitment, is what separates a campus that offers counseling from one that is genuinely trauma-informed.
Questions to Ask Yourself
Step-By-Step: How to Implement Trauma-Informed Care on Campus
Implementing trauma-informed care on campus means systematically redesigning policies, physical spaces, and interpersonal practices so that every student interaction accounts for the possibility of trauma exposure. This is not a single program or workshop but an institution-wide commitment that touches admissions, residence life, academic advising, campus safety, and beyond. The process unfolds in phases, each requiring cross-departmental collaboration and measurable benchmarks.
Phase 1: Conduct a Campus-Wide Assessment
Before launching new initiatives, institutions need a clear picture of current practices and gaps. Start by reviewing existing data sources: student health surveys, counseling center utilization reports, disciplinary records, and retention statistics disaggregated by demographic groups. Many campuses already collect relevant information but have not analyzed it through a trauma-informed lens.
Search your own institution's website for published reports on student wellness or climate surveys. Offices of institutional research, student affairs divisions, and counseling centers sometimes post outcome data showing retention or GPA changes linked to specific interventions. If your campus lacks this documentation, that gap itself becomes a priority.
Phase 2: Build a Cross-Functional Leadership Team
Trauma-informed transformation requires buy-in from multiple stakeholders. Assemble a working group that includes representatives from:
- Counseling services: Clinical expertise on trauma responses and evidence-based interventions
- Residence life: Direct contact with students in living environments where crises often surface
- Title IX and Clery compliance: Legal knowledge about mandatory reporting and investigation protocols
- Academic affairs: Faculty perspectives on classroom accommodations and academic flexibility
- Student government: Peer insight into what students actually experience and need
This team should meet regularly, review assessment findings, and develop a shared action plan with specific timelines.
Phase 3: Align With Federal Guidance and Professional Standards
Trauma-informed interviewing techniques have gained traction in Title IX investigations and Clery Act compliance. The Department of Education has issued guidance documents emphasizing the importance of investigator training that accounts for how trauma affects memory, disclosure patterns, and emotional regulation. Review current Title IX training materials on your campus to determine whether they incorporate these principles.
Professional associations offer additional resources. NASPA (Student Affairs Administrators in Higher Education), ACPA (College Student Educators International), and the Clery Center maintain case study collections and toolkits documenting how peer institutions have adopted trauma-informed frameworks. These resources often include outcome data, such as improvements in student retention or reductions in repeat disciplinary incidents, that can help justify budget requests. Emerging AI tools for counseling and psychology students can also help teams streamline data collection and identify patterns in student needs.
Phase 4: Pilot, Measure, and Scale
Rather than attempting institution-wide change overnight, select one or two departments for pilot programs. A residence hall cluster, a specific academic college, or the student conduct office can serve as testing grounds. Define success metrics in advance: Are you tracking changes in GPA among participating students? Monitoring voluntary counseling referrals? Documenting how long students stay enrolled after a crisis?
After a semester or academic year, analyze pilot outcomes and refine the approach before expanding. Publish findings internally, even informally, so other departments understand what works. Transparent documentation builds institutional knowledge and sustains momentum when leadership changes occur.
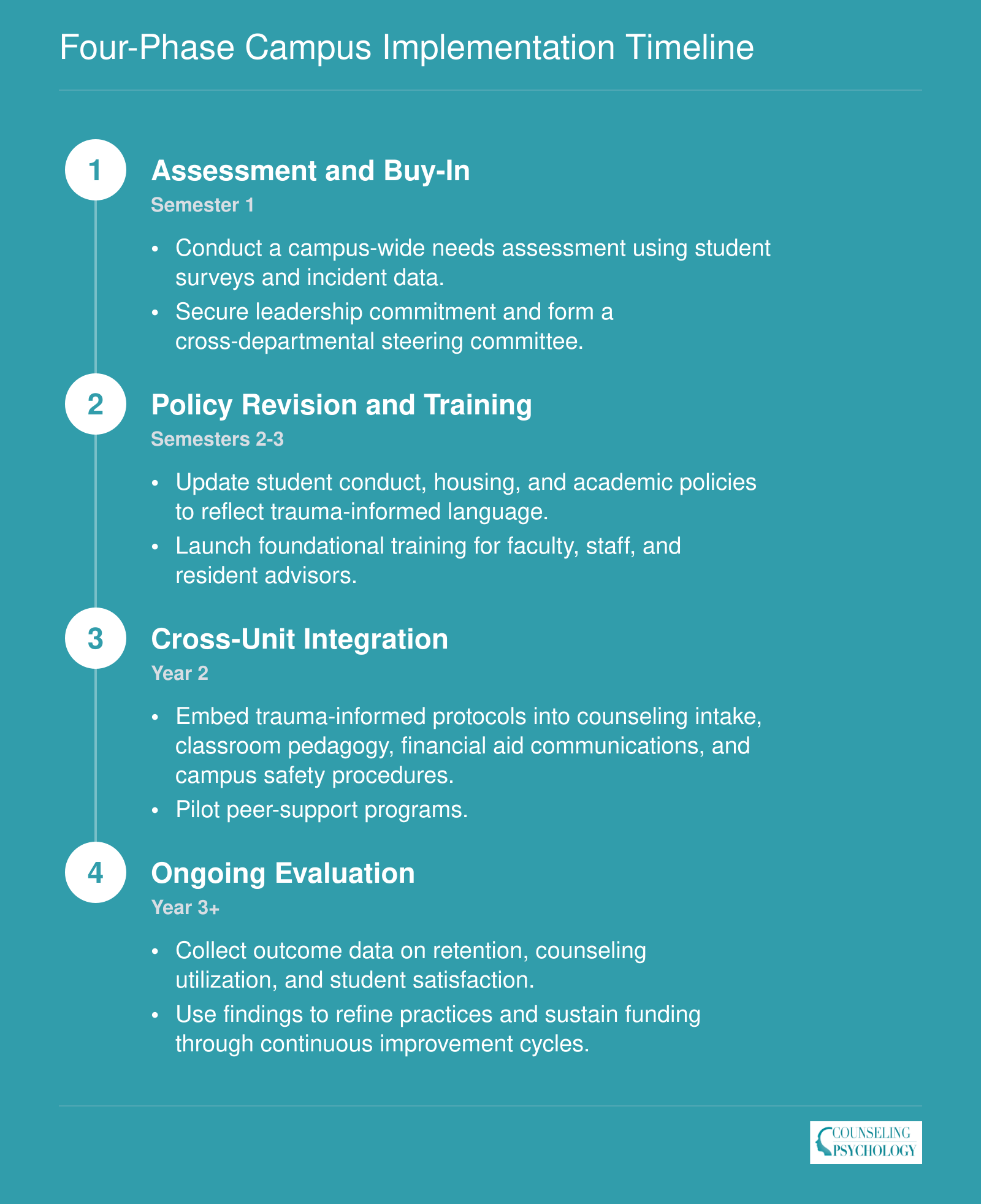
Four-Phase Campus Implementation Timeline
Moving from awareness to action takes deliberate phasing. The timeline below maps a realistic rollout that most institutions can adapt to their size and governance structure.
Trauma-Informed Practices Across Campus Settings
Trauma-informed care gains its power not from centralized policy but from daily routines in residence halls, classrooms, conduct hearings, and campus safety operations. Each setting asks staff to assume trauma is present, not exceptional, and to redesign everyday interactions so they reduce harm instead of compounding it.1 The difficulty lies in translating abstract principles into concrete protocols that frontline staff can apply under pressure.
Residence Halls
Resident advisors receive training to recognize trauma responses: freeze, fight, flight, fawn, dissociation, and shutdown.2 When a student discloses violence, self-harm, or suicidality, RAs are taught to move difficult conversations to private, quiet spaces rather than conduct triage in hallways or shared lounges.2 Housing operations increasingly provide quiet spaces or low-stimulation lounges, recognizing that sensory overload can trigger distress. Room-change policies accommodate trauma triggers, allowing students to relocate when a roommate's behavior, noise patterns, or presence creates ongoing distress. Community agreements built at the floor level encourage peer support and set norms around noise, overnight guests, and conflict, reducing the likelihood that behavior escalates to formal conduct.
Classrooms
Faculty apply universal design principles: advance notice when course material includes descriptions of violence, sexual assault, or death, paired with alternate assignments for students who need them. Flexible deadlines for crisis periods and options for incomplete grades give students temporary course relief without forcing medical withdrawal.3 Language matters. Faculty trained in trauma-informed teaching avoid inadvertent shaming ("If you cared, you'd have shown up" or "Everyone else managed to turn this in") and instead offer matter-of-fact paths forward ("Let's talk about how to catch up" or "Here's the extension form"). When a student discloses trauma during class discussion or office hours, the appropriate response is to listen briefly, affirm the courage it took to share, and connect the student to campus counseling rather than attempt to counsel on the spot.
Student Conduct
Conduct officers shift from punitive to restorative frameworks, using educational language that separates behavioral accountability from therapeutic referral.2 Trauma-informed hearing procedures allow support persons in the room, offer breaks, and avoid demanding eye contact or immediate verbal responses. When a student's behavior appears linked to trauma (substance use following assault, academic dishonesty during a mental health crisis), the outcome includes mandatory counseling referrals but treats the infraction as a teaching moment rather than a character indictment.
Campus Police
Crisis intervention specialist training teaches officers to treat mental health calls as medical or psychological crises, not disciplinary matters.4 De-escalation protocols prioritize calm tone, physical distance, and avoiding sudden movements. Warm handoffs to counseling mean an officer walks a student in distress directly to the counseling center or waits with them until a clinician arrives, rather than issuing a report and departing. Wellness checks, often requested by worried parents or roommates, follow scripts designed to avoid re-traumatization: knock gently, identify yourself clearly, explain why you are there, and ask permission to enter rather than forcing entry unless imminent danger is evident.
Trauma-informed care does not lower academic standards; it removes unnecessary barriers so students can meet those standards. When faculty raise concerns about rigor, this distinction matters: flexible policies, trigger warnings, and supportive communication help students access learning rather than excuse them from it. The goal is equity in opportunity, not reduced expectations.
Identity-Specific Considerations: LGBTQ+ Students, Students of Color, Veterans, and More
Trauma-informed care on campus must adapt to the lived realities of students who navigate multiple, intersecting forms of marginalization and adversity. Generic interventions often miss the mark when they ignore identity-specific stressors, from minority stress and racial trauma to the challenges of military-to-civilian transitions. Effective trauma-informed programming starts by acknowledging how different communities experience trauma and tailoring policies, training, and support structures accordingly.
LGBTQ+ Students: Minority Stress and Institutional Affirmation
LGBTQ+ college students report higher rates of adverse childhood experiences, including bullying, parental rejection, and harassment linked to their identities.12 On campus, discrimination and microaggressions continue that trauma trajectory, a dynamic known as minority stress.3 Trauma-informed care for this population centers on institutional affirmation: chosen-name and pronoun policies embedded in registration and learning-management systems, restrooms and locker rooms that align with gender identity, and health centers staffed by providers trained in identity-affirming care.4 Campus programming should include visible safe-space indicators, confidential reporting pathways, and access to gender and sexuality alliances (GSAs).4 Care interactions should be patient-led, with explicit permission sought before physical contact, periodic check-ins throughout sessions, and a strengths-based frame that avoids pathologizing identity.1
Students of Color: Racial Trauma and Culturally Responsive Counseling
Racial trauma, the cumulative psychological impact of racism, discrimination, and microaggressions, affects students of color at rates and in ways often invisible to majority-white campuses.3 Colorblind policies ("we treat everyone the same") can re-traumatize by denying the lived reality of race-based harm. Trauma-informed campuses adopt an intersectional framework that names racism as a traumatic stressor.4 Key interventions include counseling models informed by racial identity development theory, staff training on recognizing and responding to racial trauma, rapid institutional responses to discriminatory incidents, and culturally matched referral networks.3 Counselors and support staff should understand how trauma symptoms may present differently across cultural contexts and avoid defaulting to Eurocentric diagnostic norms. For a closer look at the landscape, including how few practitioners share the racial and ethnic backgrounds of the students they serve, see our overview of BIPOC therapists in the United States.
Student Veterans: Military Transitions and Peer Support
Student veterans arrive on campus with potential exposure to combat trauma, military sexual trauma, and the disorienting transition from rigidly hierarchical military culture to open-ended civilian academia. Trauma-informed accommodations include allowing veterans control over classroom seating (near exits, backs to walls), predictable routines, clear explanations of assignments and grading, and collaborative planning that mirrors the structured decision-making familiar from service.1 Peer-support models, such as campus chapters of Student Veterans of America, provide a bridge between military and campus norms. Counseling centers should offer rapid linkage to trauma-focused evidence-based treatments when appropriate and avoid re-traumatization through intrusive intake questions.1 Students and practitioners interested in this specialty can explore pathways through veterans counselor degree programs.
First-Generation and Low-Income Students: Financial Insecurity as Trauma Trigger
Poverty-related adverse childhood experiences (unstable housing, food insecurity, exposure to community violence) shape many first-generation and low-income students' baseline stress levels. On campus, financial insecurity acts as an ongoing trauma trigger. Trauma-informed financial-aid and housing offices reduce bureaucratic barriers, use plain language in communications, offer flexible payment options, and train staff to understand how shame and hypervigilance around money can manifest as avoidance or defensiveness. Emergency aid funds, campus food pantries, and housing-insecurity liaisons can buffer against re-traumatization.
Intersectionality: Avoiding Siloed Support
Many students hold multiple marginalized identities (a Black transgender veteran, a first-generation Latina lesbian), and their trauma exposure and needs reflect that intersectionality. Campus programs that silo support by single identity markers miss the complexity.4 Trauma-informed care applies an intersectional lens across all work, ensuring that training topics include identity-affirming communication, that reporting systems protect confidentiality without forcing students to choose between resources, and that referral networks understand overlapping identities.4 Programs designed for one group should actively welcome and adapt to others rather than assume a monolithic experience within any identity category.
Training Faculty, Staff, and Student Leaders
Building a trauma-informed campus requires intentional development of competencies across all personnel tiers. Effective training moves participants through a four-stage competency model: awareness of trauma prevalence and impact, knowledge of core principles and neurobiology, skill in applying trauma-informed communication and de-escalation techniques, and integration into daily practice and institutional policy. Programs targeting faculty, administrative staff, residential life teams, and student leaders each emphasize different points along this continuum, with the ultimate goal of embedding trauma-sensitive approaches into every campus interaction.
Validated Training Curricula
Several evidence-based programs have been adapted for higher education contexts. Columbia College offers Building Resilience Through Trauma-Informed Practices in Higher Education, an eight-week online course designed specifically for higher education professionals who wish to deepen their understanding of trauma's systemic effects on learning and student success.1 The Texas Institute for Excellence in Mental Health provides a free, two- to four-hour online Trauma-Informed Care Course suitable for all organizational staff, covering foundational principles and practical responses.2 The Ohio Department of Education's Trauma-Informed Digital Training Series, also free and available online, targets educators and staff with modules on recognizing trauma cues and creating psychologically safe classrooms.3 The University of North Carolina hosts Core Components and Skills for Trauma Informed Practice, a no-cost online resource tailored to health professionals and campus staff that emphasizes skill development in screening, empathic communication, and referral pathways.4
Additional programs widely used on college campuses include Mental Health First Aid for Higher Education, an eight-hour in-person or virtual workshop (fees vary by host institution) that trains participants to recognize signs of mental health crises and connect students with appropriate resources. QPR Gatekeeper Training teaches faculty and staff a three-step intervention (Question, Persuade, Refer) for suicide prevention counselor work in approximately 90 minutes, often offered free through campus counseling centers. Kognito produces interactive simulations in which participants practice difficult conversations with virtual students experiencing distress; licenses are purchased by institutions and made available to faculty, advisors, and residence hall staff.
Training Student Leaders Without Overstepping Boundaries
Peer-support programs extend trauma-informed awareness into student networks without requiring learners to act as unlicensed counselors. Peer health educators receive foundational training on trauma principles, active listening, and warm referral pathways. Recovery ally programs prepare students to offer non-clinical support to peers in recovery from substance use or co-occurring trauma. These models emphasize role clarity: student leaders learn to recognize signs of distress, validate experiences, and connect peers to professional resources, not to diagnose, treat, or carry clinical responsibility. Regular supervision by licensed staff and clear scope-of-practice guidelines protect both peer supporters and the students they serve.
Sustaining Competencies Over Time
One-time workshops rarely yield lasting practice change. Campuses with mature trauma-informed initiatives embed refresher modules into annual professional development calendars, create communities of practice for ongoing case consultation, and reward trauma-informed teaching with recognition in tenure and promotion criteria. When training becomes a continuous thread rather than a single event, competencies move from individual awareness into institutional culture.
Measuring Impact: Evaluating Trauma-Informed Campus Initiatives
More than 300,000 administrations of the Attitudes Related to Trauma-Informed Care (ARTIC) Scale have been completed across service settings, making it one of the most widely used instruments for tracking organizational readiness and staff development in trauma-informed work.1 Campuses that invest in training and policy changes need clear metrics to know whether those efforts translate into meaningful outcomes for students and staff alike.
Key Performance Indicators Worth Tracking
Effective evaluation begins with selecting the right indicators. Consider tracking these five metrics on an annual basis:
- Counseling utilization rates: Monitor both overall appointments and, where ethical guidelines permit, whether students with trauma histories are accessing services. Increases often signal that stigma is decreasing and help-seeking feels safer.2
- Re-enrollment and retention of at-risk students: Compare persistence rates for students flagged through early-alert systems before and after trauma-informed programming launches.
- Conduct recidivism: Track whether students who complete restorative or trauma-informed conduct processes are less likely to repeat policy violations.
- Student satisfaction survey scores: Campus climate surveys that include questions about psychological safety and belonging offer a window into how students experience the environment.3
- Staff confidence in handling disclosures: Pre- and post-training knowledge assessments reveal whether faculty and staff feel better equipped to respond appropriately when students share difficult experiences.
Assessment Tools That Work
The ARTIC Scale, developed by the Traumatic Stress Institute, is available in three versions: the ARTIC-45 (seven subscales), ARTIC-35 (five subscales), and ARTIC-10 (a single global score).4 Validation research with 1,395 providers found acceptable to excellent internal consistency and medium effect sizes for construct validity.5 The California Evidence-Based Clearinghouse rates ARTIC as "A," meaning psychometrics are well-demonstrated.6 Campuses can use the education-specific version to assess readiness before a training initiative, measure change immediately afterward, and gauge long-term sustainment.
Beyond ARTIC, standard campus climate surveys can incorporate items on psychological safety and sense of belonging. Screening tools such as the PHQ-9, GAD-7, and brief PTSD checklists help counseling centers monitor aggregate trends in student mental health. Help-seeking attitude scales add another layer by revealing whether students view campus resources as accessible and trustworthy.
What the Evidence Shows So Far
Published studies confirm that trauma-informed first-year seminars and trauma-focused counseling groups are associated with improved GPA, stronger persistence, and higher service utilization.3 However, no peer-reviewed research yet links campus-wide ARTIC scores directly to institution-level retention or counseling metrics.3 Campuses should treat ARTIC as a staff-development barometer rather than a student-outcome predictor until more longitudinal data emerge.
A Simple Annual Review Cycle
Building evaluation into the academic calendar keeps the work sustainable. Collect data each spring, when campus climate surveys typically run and counseling utilization figures close out for the year. Present findings to leadership each summer, giving administrators time to digest results before budget decisions. Use the fall semester to adjust programming, refine training content, and reallocate resources based on what the data reveal. Repeating this cycle year over year creates a feedback loop that keeps trauma-informed care from becoming a one-time initiative and instead supports an evolving campus commitment.
According to the CCMH 2024 Annual Report, roughly 45.5 percent of students who visited a college counseling center reported a history of trauma at intake. That means nearly half of all students walking through the door carry experiences that directly shape how they learn, connect, and cope on campus.
Careers in Trauma-Informed Campus Work
What jobs on a college campus actually use trauma-informed care every day, and what credentials do you need to land them?
If you have found this guide valuable as a student, you may already be building the foundation for a career in campus mental health and student support. Professionals in these roles translate trauma-informed principles into daily practice, shaping how institutions respond to student needs.
Campus Counselor or Psychologist
Clinicians working in college counseling centers conduct intake assessments, provide individual and group therapy, and respond to students in crisis. They screen for trauma histories, deliver evidence-based treatments like cognitive processing therapy, and train residence life staff on recognizing warning signs. Most positions require a master's in counseling or clinical psychology, with licensed professional counselor (LPC) or licensed psychologist credentials depending on the state. Some centers hire clinical social workers holding the LCSW. If you are exploring broader options in the field, a look at careers in psychology can help you compare related paths.
Dean of Students Office Staff
Case managers and student support coordinators in the Dean of Students office serve as bridges between academic departments, counseling services, and community resources. They coordinate care for students navigating academic disruptions tied to trauma exposure, manage behavioral intervention teams, and ensure follow-up after critical incidents. A master's in higher education administration, counseling, or social work provides strong preparation. Licensure is not always required, though an LCSW or LPC enhances advancement prospects.
Residence Life Coordinator
Residence life professionals are often the first campus employees to observe changes in student behavior. They respond to roommate conflicts, mental health emergencies, and disclosures of abuse or assault. Trauma-informed coordinators approach these situations with curiosity rather than judgment, prioritizing safety and connection. A master's in higher education or student affairs is typical, and some institutions prefer candidates with counseling backgrounds.
Title IX Investigator
Title IX staff investigate complaints of sexual harassment and assault, processes that can be retraumatizing for survivors if handled poorly. Investigators trained in trauma-informed interviewing techniques ask open-ended questions, allow for memory gaps, and avoid language that implies blame. Backgrounds in social work, law, or higher education administration are common. While licensure is not mandatory, credentials like the LCSW signal relevant clinical knowledge.
Student Wellness Program Director
Wellness directors oversee prevention programming, peer education initiatives, and campus-wide campaigns addressing mental health stigma. They analyze student survey data to identify emerging needs and collaborate with counseling centers to close service gaps. A master's in public health, counseling, or higher education administration prepares candidates well.
Salary and Job Outlook
Nationally, substance abuse, behavioral disorder, and mental health counselors earned a median salary of $59,190 in 2024, with projected job growth of 17 percent through 2034.1 Social workers across all settings earned a median of $61,330, with 6 percent projected growth over the same period. For a deeper breakdown of pay by degree level and specialty, review current counselor salary data. Salaries in educational services can vary by region and institution type, so researching specific campus postings helps set realistic expectations.
From Student to Professional
Reading about trauma-informed care now gives you a head start. You are learning the language, the principles, and the rationale that employers expect new hires to understand. Whether you pursue an MSW (and wonder whether an MSW is a terminal degree), a counseling degree, or a path in higher education leadership, this foundation positions you to advocate for students the way you wish someone had advocated for you.
Frequently Asked Questions About Trauma-Informed Care on Campus
These are some of the most common questions students, faculty, and administrators ask when exploring trauma-informed care in higher education. Each answer offers a concise starting point, though the full picture often depends on your campus context and the populations you serve.