What you’ll learn in this article…
- Therapist identity accounts for 5-8% of outcome variance, while treatment type contributes at most 1%.
- Bruce Wampold noted there are 10,000-15,000 psychotherapy trials but only about 20 studies of therapists.
- Shortages force families to accept any therapist, obscuring the wide variation in practitioner effectiveness.
When a teenager's anxiety spirals, the first instinct is to find a therapist who offers cognitive behavioral therapy or dialectical behavior therapy. But a growing body of research suggests the label matters far less than the person delivering it.
The United States is facing a teen mental health crisis, with over 40% of high school students reporting persistent sadness or hopelessness, and provider shortages mean families often wait months for an appointment. Yet even when they get one, the quality of care they receive is largely a gamble.
Like the "Widget Effect" that once masked teacher effectiveness in schools, mental health providers are treated as interchangeable parts. The scarcity distorts the market, erasing any incentive to measure or improve therapist performance. For teens in distress, that means a system built on hope rather than evidence.
The Teen Mental Health Crisis by the Numbers
A Snapshot of Teen Mental Health Today
The scale of mental distress among young people has grown from a quiet concern to a full-blown public health emergency. According to the latest Youth Risk Behavior Survey (YRBS) from the CDC, 40% of U.S. high school students reported persistent feelings of sadness or hopelessness in 2023, nearly double the rate from a decade earlier.1 Among the same group, 20% seriously considered suicide, 16% made a suicide plan, and 9% attempted suicide.1 For the 12 to 17 age bracket, national data from the National Survey on Drug Use and Health (NSDUH, reported by SAMHSA) shows that 18.1% experienced a major depressive episode in 2023, with 11.3% classified as having severe impairment in 2024, roughly 2.8 million adolescents.2
Anxiety symptoms affect an estimated one in five adolescents (20%), and depression symptoms touch close to 18%.1 These numbers are not isolated statistics; they translate into overloaded crisis lines, packed school counseling offices, and families searching desperately for appointments.
Emergency Departments and the Capacity Crunch
The surge in mental health emergencies among children and adolescents has overwhelmed hospital emergency departments. While exact figures vary by region, multiple reports confirm that hospitals frequently have to board patients waiting for inpatient psychiatric beds, sometimes for days. A teen in crisis often encounters a system where available therapists and specialized beds are scarce, turning what should be a responsive safety net into a high-stakes bottleneck. This mismatch between rising need and stagnant or shrinking provider capacity creates a crisis that deepens with every delayed appointment, which is why understanding the states with the highest need for counselors matters for workforce planning.
Disparities That Magnify the Burden
The burden of poor mental health does not fall evenly. LGBTQ+ high school students face staggeringly higher rates: 65% reported persistent sadness or hopelessness in 2023, and 41% seriously considered suicide, rates roughly double those of their non-LGBTQ+ peers.3 These youth also navigate unique barriers to care, including discrimination, lack of affirming providers, and family rejection, which compound the basic difficulty of finding an available therapist.
While nationally representative data on racial and ethnic disparities in teen mental health is often less complete, available evidence points to significant gaps. Youth from Black, Latino, and Indigenous communities frequently report higher rates of attempted suicide than their white peers, yet they are far less likely to receive mental health services. Factors such as insurance gaps, cultural stigma, language barriers, and a workforce that lacks racial and ethnic diversity contribute to unmet needs. The growing demand for BIPOC therapists underscores this inequity. The Annie E. Casey Foundation has noted that teens of color are often diagnosed later and receive less follow-up care.3
A Public Health Emergency, Not an Inconvenience
When 20% of adolescents have unmet mental health care needs (as reported in the 2021 to 2023 period) and only 20% received therapy, the system is clearly failing.1 Over half of teens (55%) discussed mental health with a healthcare provider, yet many still could not access timely, effective treatment.1 These numbers frame the provider shortage not merely as a logistical headache for families, but as a full-scale public health emergency. The following sections will explore how that shortage plays out geographically, what drives it, and why even when therapists are available, their effectiveness varies so widely that it demands a new approach to measuring quality.
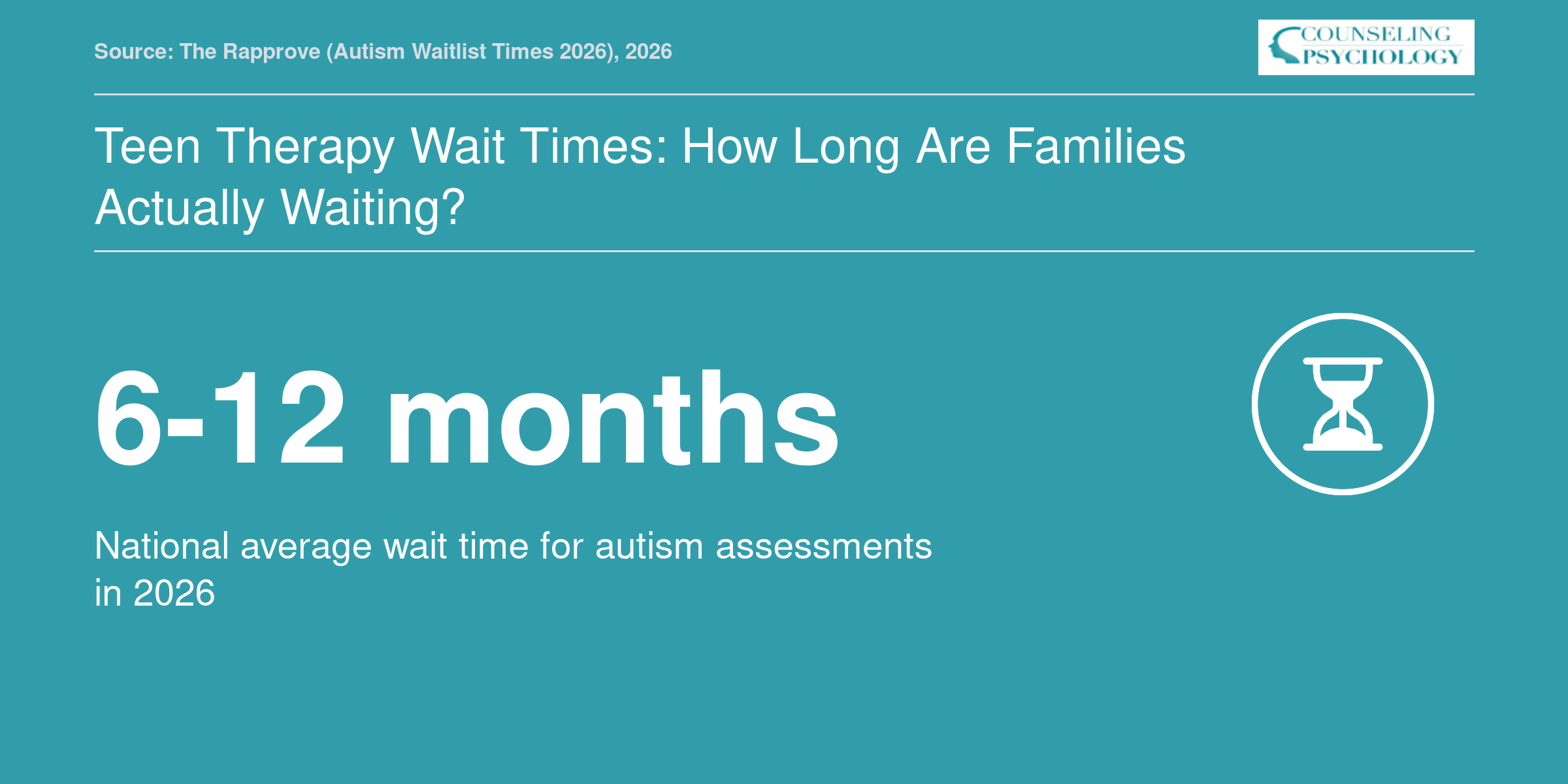
Teen Therapy Wait Times: How Long Are Families Actually Waiting?
Finding a therapist for a teenager can mean navigating long waitlists. While exact times vary by location and insurance, families can contact clinics directly, check professional association resources, or ask school counselors for the most current local information.
Which States Have the Worst Teen Mental Health Provider Shortages?
A teen's access to mental health care depends dramatically on where they live, and in several states, the odds of getting timely, effective help are stacked against them.
Measuring Access: Unmet Need and Provider Gaps
Mental Health America's annual report tracks youth mental health across all 50 states and Washington, D.C., using indicators such as the percentage of young people with major depression who did not receive any treatment.1 Nationally, more than half of youth with depression (50.8%) had unmet mental health needs in the most recent dataset.1 The overall provider ratio sits at roughly 340 people for every one mental health provider, but that average masks extreme variation.2 When zooming in on adolescents specifically, about 20% go without needed care, a figure that balloons in certain regions.3 These trends are part of the broader mental health workforce shortage reshaping the counseling profession nationwide.
These metrics combine to reveal clear geographic winners and losers. States that consistently appear at the bottom share patterns of low provider density, high youth-per-provider ratios, and widespread Health Professional Shortage Area (HPSA) designations for child and adolescent psychiatry.
States With the Most Severe Shortages
Based on the most recent tiered rankings, the worst access for teen mental health care clusters in the South and parts of the Mountain West.1 Five states stand out for their persistently low rankings across multiple years:
- Alabama: Reports one of the highest percentages of youth with unmet mental health needs, hovering around 66%.4 The state's provider pipelines are thin, and rural counties face extreme travel barriers.
- Arizona, Nevada, and Montana: All three land in the lowest overall mental health tier.2 Nevada's youth preventive care ranking sits at 51st, indicating systemic gaps that affect early intervention for teens.1 Arizona and Montana share challenges tied to geographic isolation, Medicaid reimbursement rates, and limited training programs.
- Texas and Georgia: Both states have large overall populations but fail to meet teen mental health demand. Unmet need among youth with depression exceeds 55% in each, driven partly by uneven distribution of specialists concentrated in urban centers while huge swaths of rural and suburban families face desert-level shortages.1
- Mississippi and South Carolina: These states, along with others in the bottom tier, consistently show youth-to-provider ratios far above the national average, compounded by high poverty rates and fewer school-based mental health services.1
What's Driving the Shortage in These States?
Geography is a primary culprit. Vast rural stretches in Montana, Nevada, and parts of Alabama create practical obstacles: families might drive over an hour to reach the nearest adolescent therapist, and telehealth can only partially bridge the gap when broadband access is inconsistent. Medicaid policy also shapes workforce size. States that have not expanded Medicaid or that reimburse behavioral health providers at low rates struggle to attract and retain practitioners. Finally, training pipelines matter. The bottom-ranking states tend to have fewer psychiatry residency slots and accredited counseling psychology programs, so new professionals often leave for regions with better pay and support. Understanding which psychology specialists are most needed can help aspiring clinicians direct their training toward the greatest gaps.
Disparities That Deepen the Crisis
State-level rankings also interact with identity-based access gaps. LGBTQ+ teens in states with the worst provider shortages frequently face dual barriers: a dearth of clinicians trained in affirming care and cultural climates that discourage help-seeking. Similarly, Black and Latino adolescents in these states are more likely to attend under-resourced schools and encounter providers who lack cultural competence, turning unmet need into an equity emergency. The intersection of location, race, and sexual orientation means that a teenager in a bottom-tier state who is also a minority faces far worse odds of receiving quality care than numbers alone suggest.
Ask Yourself
Understanding the Provider Shortage: Who Treats Teens and Where Are the Gaps?
Teens in crisis often need specialized, developmentally attuned care, yet the professionals trained to deliver it are spread dangerously thin. Understanding who works in this space, and where the gaps emerge, is the first step toward seeing the shortage not as a vague crisis, but as a set of solvable pipeline and distribution problems.
The Professionals on the Front Lines
Teen mental health care draws from several licensed professions, each with distinct training paths. Child and adolescent psychiatrists are medical doctors who complete a four-year psychiatry residency followed by a two-year fellowship in child and adolescent psychiatry. Psychologists typically earn a doctorate degree in psychology (PhD or PsyD), often with specialized clinical training in youth populations. Clinical social workers hold a master's degree in social work (MSW) and may pursue postgraduate hours toward licensure as a Licensed Clinical Social Worker (LCSW), sometimes concentrating in school-based or family services. Licensed professional counselors (LPCs) and marriage and family therapists (MFTs) also complete master's programs and direct clinical hours, and many focus on adolescent practice. School counselors, school psychologists, and pediatric primary care providers further extend the safety net, particularly for earlier intervention and referral.
Despite this workforce breadth, the pipeline into teen-focused specialties is narrow. Child and adolescent psychiatry fellowships produce a small annual cohort; interest in these training slots far exceeds capacity. Social work and counseling programs graduate many generalist practitioners, but formal concentrations in youth and adolescent mental health remain limited, leaving many new clinicians to learn on the job. The result is a persistent mismatch between the number of teens seeking care and the availability of clinicians with developmentally appropriate expertise. Understanding which counseling specialties most in demand can help prospective clinicians direct their training where the need is greatest.
Where the Gaps Hit Hardest
Geography magnifies the shortage. Rural and frontier counties often lack any board-certified child psychiatrist, forcing families to travel hours or rely on telehealth, if broadband access permits. Low-income urban neighborhoods may have community mental health centers, but waitlists stretch months, and therapists frequently manage caseloads two to three times the recommended size. Schools, where teens spend the bulk of their waking hours, have long been understaffed: the recommended ratios for school psychologists and school counselors are rarely met, leaving many students without on-site support.
The shortage also skews toward early-career clinicians. Without structured mentorship or manageable caseloads, burnout drives premature attrition, shrinking the available workforce just as the need peaks. Projected retirements of older practitioners, many of whom entered the field decades ago, threaten to compound the gap over the next ten years.
Tracking the Numbers Yourself
For those wanting to monitor or advocate around training pipelines, public data sources can help. The American Academy of Child and Adolescent Psychiatry (AACAP) maintains lists of accredited fellowship programs and occasional workforce reports. The Council on Social Work Education (CSWE) publishes annual statistics on enrollment and graduation, including some breakouts by practice concentration. National workforce projections for mental health occupations are available through the Bureau of Labor Statistics (BLS) Occupational Outlook Handbook. And because aggregated data often lag, direct contact with university departments of psychiatry, psychology, and social work can yield the most current class sizes and graduation trends. Without sustained investment in these training pipelines, the disconnect between the providers teens need and the providers available will only deepen.
What Is the Therapist Widget Effect?
The effectiveness of your therapist depends far more on who they are than on the specific therapy model they use, but the mental health profession largely treats clinicians as interchangeable parts. The result is a system that defaults to assuming all licensed therapists deliver equivalent care, a dangerous assumption when teens are waiting months for help.
The Widget Effect in Education
The term "widget effect" comes from a 2009 report by The New Teacher Project, which examined how public school systems evaluated teachers.1 The report found that schools treated teachers as interchangeable widgets, rarely differentiating between high and low performers, providing minimal feedback, and almost never dismissing anyone for ineffectiveness. As a result, teacher quality was assumed rather than assessed, and student outcomes suffered. In the years since, education reformers have pushed for more rigorous evaluation systems, though progress remains uneven.
The Same Pattern in Psychotherapy
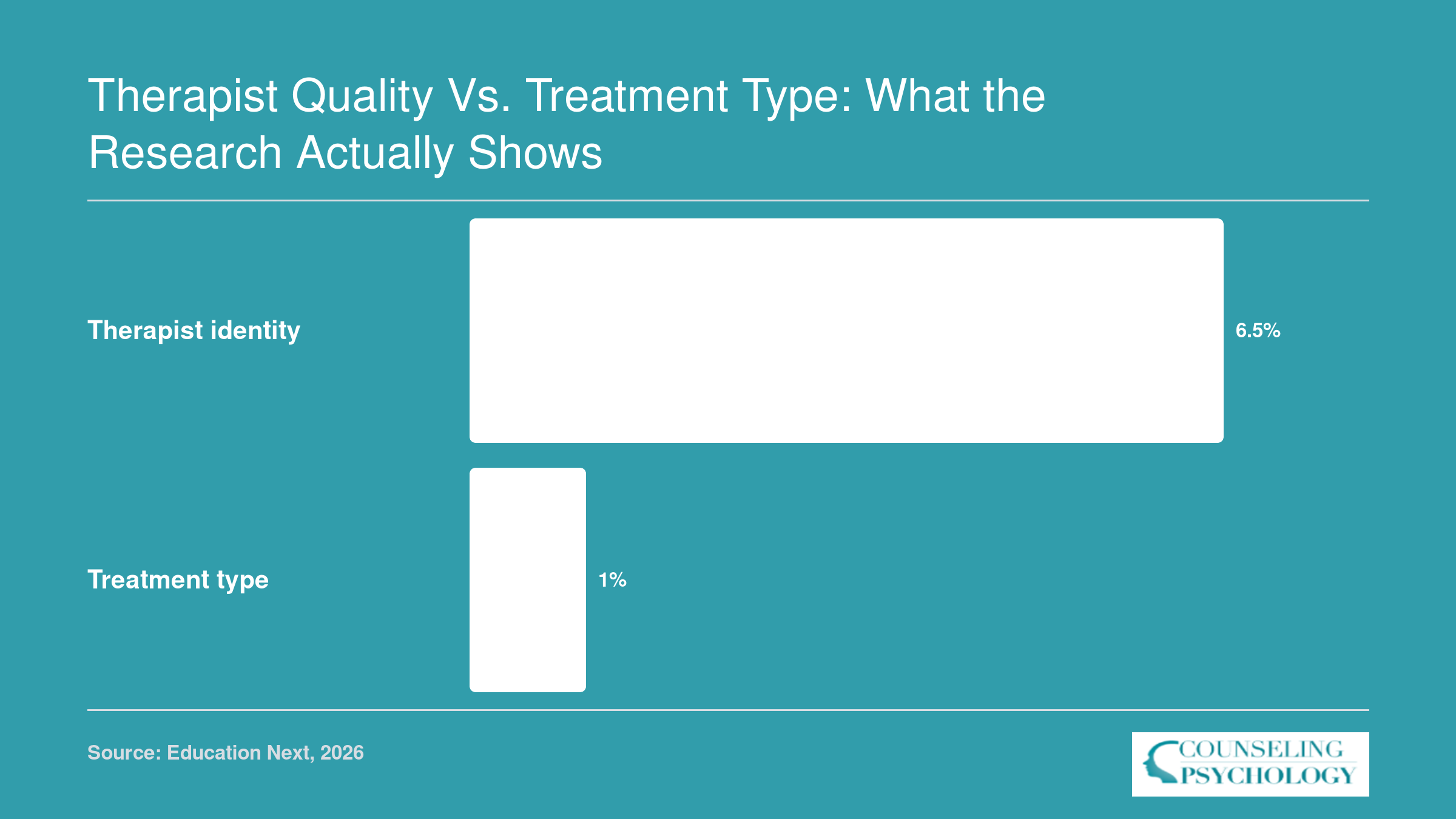
Bruce Wampold, emeritus professor of counseling psychology at the University of Wisconsin and director of the Research Institute at Modum Bad Psychiatric Center in Norway, argues that psychotherapy exhibits the same widget effect. His research shows that the identity of the therapist accounts for roughly 5 to 8% of the variance in patient outcomes.1 By contrast, the type of treatment a therapist delivers, whether cognitive behavioral therapy, psychodynamic therapy, or any other evidence-based modality, accounts for at most 1% of outcome variance. In plain terms, whether your therapist is effective has little to do with which manualized treatment they follow. It comes down to the therapist themselves: their ability to build a working alliance, their interpersonal skills, their capacity for nuanced clinical judgment.
Yet as Wampold notes, the profession behaves as if the opposite were true. Training programs emphasize mastery of specific treatment protocols. Counseling licensure acronyms and credentials dominate how clinicians present their qualifications, while licensure itself focuses on passing exams and completing supervised hours. Continued education requirements revolve around accumulating credits, often in preferred modalities. The implicit message: all therapists who hold a given license are roughly equivalent in skill. That assumption collapses under the weight of the outcome data.
A Parallel Accountability Vacuum
The parallel with education is striking. In a large-scale analysis across 24 states, researcher Matthew Kraft found that fewer than 1% of teachers were rated in the lowest evaluation category, suggesting that poor performance is simply not identified through current systems.1 Therapists face an even more complete accountability vacuum. As Wampold bluntly stated, "There is no other profession where your performance is so ignored as psychotherapy." There have been 10,000 to 15,000 clinical trials comparing different psychotherapies, but perhaps only 20 studies have directly compared individual therapists. The National Institute of Mental Health denied Wampold's funding proposal to study therapist effects, signaling how little investment exists in understanding what makes a therapist effective.
For families seeking help for a teenager in crisis, this vacuum has real consequences. A parent can spend months getting an appointment, only to land with a therapist who may or may not be effective, and no readily available information distinguishes one from another. Advanced degrees and additional certifications, the research consistently shows, are weak predictors of actual patient outcomes. Even years of experience offer no guarantee: a longitudinal study following 170 therapists over up to 18 years found that therapist effectiveness drifted slightly downward with experience, even after researchers David Saxon and Michael Barkham controlled for case severity and patient risk.1
A Call to Measure What Matters
This is not an indictment of therapists as dedicated professionals. It is a call for the field to do what other high-stakes professions do: systematically measure outcomes and use that data to support, develop, and, when necessary, remove practitioners. The growing demand for therapists makes this even more urgent. Without routine outcome monitoring, therapy remains a black box, and the shortage of adolescent providers makes it even harder to direct teens toward clinicians who can truly help. The widget effect doesn't mean therapists are widgets; it means the system treats them that way, and teens pay the price.
Therapist Quality vs. Treatment Type: What the Research Actually Shows
The source of a teen's improvement depends far more on which therapist they see than on the specific treatment model used. Advanced degrees and certifications predict outcomes weakly, and a long-term study of 170 therapists found effectiveness actually drifted slightly downward with experience, even after controlling for case severity (Saxon & Barkham).
Why Therapist Effectiveness Is So Rarely Measured
If you searched for a surgeon, you could in many states find comparative data on infection rates and patient outcomes. If you evaluated a school, you might consult teacher-level impact metrics. But if you are a parent trying to find an effective therapist for your teenager, you enter a data vacuum. The field of psychotherapy has collectively failed to measure or report how well individual clinicians actually perform. This is not an oversight. It reflects decades of research priorities, funding decisions, and systemic habits that have ignored the person delivering the care.
The Staggering Disparity in Research
Bruce Wampold, emeritus professor of counseling psychology at the University of Wisconsin, points to a startling imbalance. There have been an estimated 10,000 to 15,000 clinical trials comparing different types of psychotherapy, such as cognitive behavioral therapy versus psychodynamic approaches.1 In that same period, Wampold notes, perhaps 20 studies have examined individual therapists as the unit of analysis. The profession has invested enormously in proving that treatments work, while neglecting the evidence that some clinicians consistently produce better outcomes than others, regardless of the method they use.
A System Designed to Study Treatments, Not Treaters
This gap is not accidental. When Wampold and his colleagues applied to the National Institute of Mental Health for funding to study therapist effects, they were denied.1 The default expectation at major research funders is that proposals will compare treatment protocols, not providers. The scientific infrastructure, from grant review panels to academic promotion standards, favors manualized treatment comparisons. Studying therapists is seen as messy, hard to control, and less prestigious. The result is a self-perpetuating cycle: without funding, the evidence base on what makes a therapist effective cannot grow.
Structural Barriers in Everyday Practice
Beyond research, everyday clinical settings do little to track outcome data. Most outpatient therapists, including those treating adolescents, never use routine outcome monitoring tools that would measure symptom change session by session. Standardized therapist-level reporting does not exist. Even when agencies collect data, it is rarely aggregated or shared publicly because of legitimate privacy concerns about small sample sizes per clinician and strong professional resistance. Many therapists fear that comparative data could be misused by insurers or could undermine the therapeutic alliance.
Psychotherapy Lags Behind Other Professions
In medicine, surgeon report cards and hospital quality dashboards are increasingly common. In education, teacher value-added models and observations aim to differentiate performance, however imperfectly. Psychotherapy, by contrast, treats practitioners as largely interchangeable. The famous Widget Effect report from 2009 highlighted how schools treated teachers as interchangeable parts.1 The same pattern holds in mental health. Credentials and experience are used as proxies for quality, despite evidence that they explain almost no variance in patient outcomes. For students weighing their options, the real question is not just whether becoming a therapist is worth it but whether the profession will build the accountability structures to match its aspirations. The field clings to the illusion that if a therapist is licensed and trained in an evidence-based treatment, the result should be uniformly good, a belief that the data does not support.
What This Means for Parents Seeking Teen Therapy
For a parent looking to help a distressed teenager, the absence of therapist-specific outcomes is profoundly disempowering. You can find a therapist who lists a specialty in adolescent issues, but you have no way to know whether that clinician actually helps most teens improve quickly, or at all. Understanding the difference between LPC and therapist credentials, for instance, tells you about training paths but reveals nothing about measured effectiveness. The teen mental health crisis makes this gap urgent. When waitlists are long and a teenager is suffering, families must make decisions based on profiles, word-of-mouth, and availability, never on measured effectiveness. The field's reluctance to measure and report therapist-level outcomes leaves parents navigating a high-stakes choice in the dark.
Key Insight: The Shortage Makes the Quality Problem Worse
In a tight market, families are forced to accept whoever has an opening, making therapist quality a luxury few can prioritize. This scarcity doesn't just mean fewer appointments; it erases the consumer pressure that could drive systematic measurement of effectiveness, leaving the field with no reliable way to distinguish good therapists from ineffective ones.
How the Shortage Compounds the Quality Problem for Teens
The persistent shortage of teen mental health providers does more than stretch appointment calendars. It systematically erodes the conditions that would otherwise push the field toward measuring and improving quality.
When Access Is Scarce, Quality Becomes Invisible
In a functioning marketplace, families vote with their feet. They leave an ineffective therapist and seek a better match. But when waitlists stretch to months and every provider in a 50-mile radius is full, that choice evaporates. The scarcity removes the consumer pressure that drives clinics, group practices, and solo practitioners to demonstrate, or even track, their outcomes. When demand far exceeds supply, the incentive to prove effectiveness disappears, and the field settles into a comfortable but dangerous assumption: that any therapy is good therapy.
This cycle is self-reinforcing. Without routine outcome measurement, therapists never see how they compare. Research shows therapist identity accounts for 5-8% of variance in patient outcomes, while treatment type contributes at most 1%.1 Yet the system rarely measures that individual impact. The result is an information vacuum where families cannot tell which providers move teens toward recovery and which leave them stuck.
Rural and Underserved Teens Face a Double Disadvantage
In rural counties and federally designated shortage areas, teens confront both a numeric shortage and a complete absence of performance data. The nearest therapist may be the only therapist. Even if that provider is deeply caring, no one, including the therapist, knows whether their work produces typical, above-average, or below-average results. The double disadvantage means families must gamble, and teens with severe presentations have no empirical basis to choose a provider equipped to handle complex cases. The states with highest need for psychologists often overlap with these underserved regions, compounding access barriers.
Insurance Networks Narrow the Window to Effective Care
Insurance paneling adds another layer. A family who researches, verifies, and identifies a therapist with a strong reputation may discover that provider does not accept their plan, or has closed their panel because reimbursement rates lag. The network then narrows to a handful of options, none of which have publicly reported effectiveness data. Narrow networks remove the very few high-quality signals families could act on, and therapists inside those networks receive no systematic feedback on their work.
Cultural Competence: A Hard-to-Measure Dimension That Matters
For LGBTQ+ teens and teens of color, the quality problem deepens. Cultural competence is a critical dimension of therapeutic effectiveness, yet it is even less measured than general outcomes. A therapist who achieves good results with one population may struggle with another, but no infrastructure tracks these differential effects. Teens who need identity-affirming, culturally grounded care often face the smallest pool of providers and the least information about whether those providers actually help.
Therapist Blind Spots in a System That Doesn't Give Feedback
For the clinical reader, the most unsettling consequence is this: well-intentioned, well-trained therapists may never learn they are ineffective or harmful with certain teens. A longitudinal study of 170 therapists over 18 years found that, on average, effectiveness drifted slightly downward with experience, yet no alert system flagged this decline.1 Without measurement, the field leaves therapists blind to their own performance, and teens bear the cost. The shortage turns every slot into a precious commodity, silencing the very conversations about quality that could protect the most vulnerable adolescents.
What States, Schools, and Emerging Programs Are Doing, and What's Still Missing
Most policy responses to the teen mental health provider shortage center on expanding the workforce, yet they sidestep the deeper problem that not all therapists are equally effective. Without accountability measures that differentiate therapist quality, these efforts risk treating practitioners as interchangeable: the very "therapist widget effect" that undermines care. Below, we survey four common policy levers, then highlight the rare programs that attempt to measure and lift quality.
State-Level Scope of Practice Expansions and Telehealth Policies
Dozens of states have recently broadened scope-of-practice laws, permitting school psychologists, licensed professional counselors, and even primary care clinicians to deliver therapy without traditional supervisory restrictions. Simultaneously, post-2022 telehealth expansions, initially pandemic-driven, were made permanent in many states, allowing teens to access providers across geographic barriers. Both changes meaningfully increase the number of faces in the workforce, but the evidence on outcomes is cautious. Wait-time data from large health systems suggest telehealth visits grew rapidly, yet appointment availability for new adolescent patients often remained unchanged because demand surged even faster. These quantity-side moves help, but they treat the shortage as a headcount problem and do not screen for or develop therapist effectiveness.
School-Based Mental Health Staffing Mandates
In the last three years, at least 15 states enacted or strengthened mandated student-to-counselor ratios, while others poured funding into school-based health centers. Federal grants through the Bipartisan Safer Communities Act accelerated hiring. These are important steps for early identification and access, particularly in underserved districts. Still, staffing mandates focus on numbers, not performance. Few states couple funding with measurement-based evaluation systems. Without tracking whether school therapists are helping students improve, districts cannot distinguish between highly effective clinicians and those who merely fill a seat. Early outcome data from a handful of districts that piloted routine measurement show that some therapists produce consistent gains while others leave students no better off, patterns that remain invisible in aggregate reporting.
Routine Outcome Monitoring: A Bridge to Quality
A different kind of solution is gaining ground: routine outcome monitoring (ROM). ROM involves collecting brief, standardized feedback from teen clients about their symptoms and progress at each session, then sharing that data with therapists. A 2023 synthesis of 58 studies, 49 of them randomized controlled trials, found that ROM alone boosts therapy success rates by approximately 8%.1 When therapists also use clinical support tools, prompts that help adjust treatment when a client is off track, the improvement ranges from 20% to 29%.1 Encouragingly, recent data from surveys of child and youth psychotherapists indicate that they endorse outcome measurement and are more likely to adopt it than their adult-focused peers.2 In the UK, routine outcome measurement is already embedded in Child and Adolescent Mental Health Services.3 Yet in the US, ROM remains fragmented; only a few large youth-serving systems, such as some managed care organizations and specialty clinics, systematically gather therapist-specific outcome data. Research also suggests that web-based ROM platforms can increase completion rates, making implementation more practical for busy clinicians.4
Where Quality Accountability Still Falls Short
Even within forward-looking ROM initiatives, therapist-level effectiveness scores are rarely aggregated for the public, for payers, or for professional development. The researcher-practitioner gap persists: over 10,000 clinical trials have compared treatment types, but fewer than two dozen studies have rigorously examined individual therapist differences. Advanced credentials and years of experience remain the default quality signals, despite weak links to outcomes. For students weighing graduate training options, this reality underscores the importance of continuing education for psychologists as a vehicle for ongoing skill development rather than credential collection. Without transparent, outcome-informed feedback loops, the therapist widget effect endures. Closing the teen mental health gap will require not only more boots on the ground but also systems that nurture and reward effective helpers.
Related Articles
Actionable Steps for Families, Clinicians, and Future Providers
Concrete steps to address the teen mental health provider shortage begin with a shift in focus, from merely expanding the number of therapists to making their effectiveness visible and measurable. The Widget Effect equivalent in mental health means that too often, therapists are treated as interchangeable parts, with little attention to how well they actually help teens improve. The following strategies target families seeking care, clinicians wanting to grow, and students preparing to enter the field.
For Families: How to Find and Monitor Quality Care for Your Teen
Families navigating the patchwork of teen mental health services can take proactive steps to raise the odds of finding effective care.
- Ask prospective therapists about outcome tracking. Inquire directly whether they use standardized measures, such as the PHQ-A for depression or the GAD-7 for anxiety, to monitor progress session by session. A therapist who routinely collects and reviews such data is more likely to notice when a teen is not improving and to adjust the approach accordingly.
- Use validated screeners as a family-level check. Even without a therapist, you can track your teen's symptoms over time using freely available tools. For example, the GAD-7 is a brief anxiety questionnaire; a score of 12 or higher signals moderately severe anxiety that warrants consistent follow-up.1 Comparing scores every few weeks can show whether symptoms are trending in the right direction.
- Consider telehealth to widen your search radius. Many states now participate in cross-state licensing compacts like PSYPACT, allowing psychologists to practice across state lines via telehealth. This expands your options beyond local providers with long waitlists, especially in rural or shortage-designated areas. For those interested in this growing model, our guide on how to become a telehealth therapist covers the degrees and steps involved.
- Use state-specific directories that identify teen-focused providers. Several states maintain searchable lists of licensed clinicians with verified specialties in child and adolescent mental health. These directories can help you bypass general practitioners who may lack experience with adolescent issues.
These steps empower families to become informed seekers of care, rather than passive recipients, and they begin to demand the kind of visibility that the Widget Effect obscures.
For Clinicians: Make Your Own Work Measurable
The research is clear: therapist identity accounts for roughly 5 to 8 percent of the variance in patient outcomes, while the specific treatment type accounts for at most 1 percent.1 Yet most therapists never receive systematic feedback on their effectiveness. Routine outcome monitoring can change that.
- Adopt session-by-session outcome measurement. Implementing brief standardized tools at each session, and reviewing the results, gives you a real-time signal of how a client is doing. Studies show that therapists who receive regular feedback achieve better outcomes, particularly with cases that are slow to improve.
- Frame measurement as a professional development tool, not a surveillance system. The data you collect is yours to use for your own growth. It lets you see patterns, identify blind spots, and refine your techniques. Notably, a large longitudinal study found that, on average, therapist effectiveness drifted slightly downward over up to 18 years of experience, underscoring that experience alone does not guarantee improvement.1 Outcome monitoring provides the feedback that experience lacks.
- Seek consultation based on your own outcome data. When a client's scores stagnate or worsen, use the data to structure a focused conversation with a supervisor or peer. This practice turns measurement into a collaborative, low-threat learning opportunity.
By making your work visible to yourself, you counter the Widget Effect in your own practice, moving from an interchangeable part to a continuously improving professional.
For Aspiring Counselors and Students: Opportunity Meets Accountability
The current shortage creates an urgent career opening, but it also carries a professional responsibility. For students weighing whether becoming a therapist is worth it, entering the field today means stepping into a role where the expectation to demonstrate effectiveness is rising.
- Recognize that the shortage is a mandate to be better, not just present. High demand can tempt systems to lower standards, but the data on therapist variability means that simply expanding the workforce without quality safeguards will not solve the teen crisis. As a new provider, you have the opportunity to set a higher baseline.
- Seek training programs that teach routine outcome monitoring. Ask programs directly whether they embed measurement and feedback-informed treatment into their clinical training. Graduates who are already comfortable with outcome data will be better prepared and will stand out in a field still dominated by opaque credentialing.
- Embrace being measured as a career-long practice. Advanced degrees and additional certifications are weak predictors of client outcomes.1 What matters more is your willingness to track and respond to the actual progress of the people you serve. Cultivating that habit now will make you a more effective, adaptive clinician.
Making Effectiveness Visible: The Antidote to the Widget Effect
For families, clinicians, and students alike, the path forward involves normalizing the measurement and transparency of therapeutic work. The Widget Effect flourishes when performance goes unseen; it diminishes when outcomes are tracked, shared, and used for growth. Addressing the teen mental health provider shortage requires not just more therapists, but therapists whose impact can be seen and steadily improved.