What you’ll learn in this article…
- Blue Cross Blue Shield of Michigan will restrict incident-to billing to facility-based settings on March 1, 2027.
- Limited license clinicians serving 42% of clients at one practice may lose insurance coverage.
- Over 50% of a practice's BCBSM revenue is tied to the soon-prohibited billing arrangement.
On March 1, 2027, Blue Cross Blue Shield of Michigan will end incident-to billing for limited license mental health professionals in private practice. After that date, only fully licensed clinicians, or limited license professionals working in facility-based settings like hospitals, can bill BCBSM for services.
At practices such as WillowsEdge Counseling and Healing Arts Center, 42% of clients are seen by limited license counselors, and BCBSM accounts for more than half of the practice's revenue. Across Michigan, the insurer is the dominant payer for mental health services.
The policy shift threatens to dismantle the supervision pipeline that supplies the state's future licensed workforce, while also disrupting established client relationships that often take months or years to build.
What Is the BCBSM Incident-to Billing Change?
The insurance reimbursement landscape for mental health professionals in Michigan is undergoing a significant reset. In June 2026, Blue Cross Blue Shield of Michigan (BCBSM) published a provider bulletin in its newsletter, *The Record*, that will fundamentally alter how limited license therapists can bill for services delivered in private practice settings.1 The policy change centers on "incident-to" billing, a mechanism that has long supported the supervision pipeline for counselors, social workers, and marriage and family therapists.
What Was Incident-To Billing?
Before this change, a limited license professional, such as a Limited Licensed Master Social Worker (LLMSW), Limited Licensed Professional Counselor (LLPC), or Limited Licensed Marriage and Family Therapist (LLMFT), could provide therapy under a fully licensed supervisor's National Provider Identifier (NPI). The service was billed as if the supervisor performed it, as long as state supervision requirements were met. This "incident-to" arrangement meant clients could see their therapist in private practice, the practice received BCBSM reimbursement, and the limited licensee gained required experience hours toward independent licensure. In effect, the supervisor's NPI acted as a billing umbrella, making care financially accessible when direct billing by the limited licensee was not allowed by BCBSM. For professionals weighing the distinctions among these credential paths, understanding counseling vs psychology vs social work degrees is an important first step.
The New Policy: Key Dates and Changes
Effective March 1, 2027, BCBSM will restrict incident-to billing to facility-based settings only, including psychiatric hospitals, community mental health agencies, and similar institutional environments.2 Private practice offices, regardless of size, will no longer qualify. To help providers adjust, a transition period runs from September 1, 2026, through February 28, 2027. During this window, services rendered by limited license clinicians under supervision can still be billed with the "SA" modifier, but reimbursement will be paid at the submitting provider's applicable rate and they will not be eligible for value-based incentive programs.3 After the transition, any limited licensee attempting to bill incident-to from a private practice will face a penalty: only 80% of the allowed amount will be paid, and the claim remains ineligible for value-based reimbursement.
The policy also states that after March 1, 2027, all affected providers, including advanced practice providers and limited license clinicians, must bill under their own NPI.1 This aligns BCBSM's commercial policy with its Blue Care Network arm, which never permitted incident-to billing for limited license professionals outside of facilities.4
BCBSM's Rationale and Broader Implications
BCBSM has stated that the change is part of routine policy review and is intended to ensure that members receive care from fully licensed professionals.4 On its surface, this logic prioritizes fully independent practitioners and standardizes billing across its product lines. However, it also severs a path that made supervision affordable for small practices and sustained client access for those seeing more affordable, pre-licensed therapists. Some limited license clinicians working toward full licensure may need to explore roles in community mental health settings, where facility-based incident-to billing will still be permitted.
It is important to note that BCBSM still covers mental health counseling; the change does not eliminate coverage for services provided by fully licensed counselors, psychologists, or social workers who bill under their own credentials. Direct billing by independently licensed clinicians remains unaffected. But for the many limited license therapists working in private settings, and the thousands of clients they serve, the rule marks a decisive shift that will reshape the business and training model of outpatient mental health care in Michigan.
Which License Types and Practice Settings Are Affected?
The upcoming BCBSM policy change restricts which professional settings can use incident-to billing for providers who hold a limited license. Under incident-to billing, a service provided by a limited license counselor, social worker, or therapist was submitted under the National Provider Identifier (NPI) of an on-site fully licensed supervisor, allowing the practice to be reimbursed at the supervisor's established rate.1 Starting March 1, 2027, this billing arrangement will only be allowed when the service is delivered in a facility-based setting, not in a typical private practice office.2
Limited License Types That Lose Private Practice Billing
- Licensed Professional Counselor (LLPC): Currently eligible for incident-to billing in all settings; after March 2027, restricted to facility-based sites only.1
- Licensed Master Social Worker (LLMSW): Same restriction applies; no incident-to billing in private offices.1
- Licensed Marriage and Family Therapist (LLMFT): Also loses the ability to bill incident-to outside of facility-based employers.1
- Temporary Limited Licensed Psychologist (TLLP): BCBSM has not published clear guidance for this license type. Practices employing TLLPs should contact provider relations directly to clarify billing pathways before the deadline.1
- Counseling students, trainees, and provisionally licensed individuals: These pre-licensed practitioners are also subject to the new facility-only limitation.1
What Counts as a Facility-Based Setting
BCBSM has indicated that facility-based settings include hospitals, outpatient psychiatric centers, Federally Qualified Health Centers, and certain community mental health clinics.3 These sites typically operate under a facility license or designation and employ practitioners as W-2 staff rather than as independent contractors. A private group practice operating out of leased office space, even if it provides multidisciplinary care, does not qualify as a facility-based setting under this policy.
Practices that wish to retain limited license staff after the change will need to consider whether they can reorganize as a licensed facility or partner with an existing hospital or health system to deliver services under that umbrella. However, such restructuring is not straightforward and may be out of reach for smaller, independent practices. Understanding counseling licensure requirements at the state level is an important first step for any clinician evaluating their options.
Notable Exemptions and Missing Information
The new billing restriction does not apply to Medicare Plus Blue or BCN Advantage plans, which already operate under separate incident-to rules.2 Providers who bill these plans should continue following existing guidance.
Additionally, BCBSM has not released detailed administrative definitions of what documentation a practice must maintain to prove a service was rendered in a facility-based setting. Professional associations, including the National Association of Social Workers Michigan chapter, have requested more specific operational details.1 Until those are published, practice owners should document all supervision and practice arrangements meticulously.
How the Change Impacts Private Practice Revenue and Staffing
For private practices dependent on BCBSM reimbursement, the billing change presents two harsh alternatives: find ways to absorb the loss of revenue or reduce their workforce of limited license clinicians. The math is unforgiving, and the consequences will ripple through Michigan's mental health landscape long before the March 2027 deadline.
Revenue Dependency and the WillowsEdge Example
David Sniderman, a clinical mental health counselor at WillowsEdge Counseling and Healing Arts Center, told WDIV ClickOnDetroit in June 2026 that 42% of the practice's clients are seen by limited license counselors.1 At the same time, over half of WillowsEdge's revenue flows from Blue Cross Blue Shield of Michigan. When the new policy takes effect, those two facts collide: none of those BCBSM sessions with limited license providers can be billed incident-to in the private practice setting.
For WillowsEdge and similar practices, the immediate revenue gap is not marginal. A practice losing the ability to bill for nearly half its client appointments could face a 20 to 30 percent drop in reimbursable services, depending on the exact payer mix. Because BCBSM often carries a large share of the commercial insurance market in Michigan, this pattern repeats across the state.
The Domino Effect on Staffing and Service Delivery
Once incident-to billing disappears for office-based practices, owners must decide which path to follow. They can absorb the cost by providing uncompensated care, an unsustainable choice for most small businesses, or rush to transfer clients to fully licensed clinicians. The latter path hits an immediate capacity wall: fully licensed therapists typically carry full caseloads already, and adding dozens of clients overnight is not realistic. The third, and in many cases inevitable, outcome is to lay off limited license counselors.
Katie Stetler, a social worker and medical billing specialist quoted in the same ClickOnDetroit report, expressed deep concern that mass layoffs of limited license professionals across the state are likely.1 For practices where BCBSM is the dominant payer, letting go of pre-licensed staff may be the only way to keep the doors open. That not only disrupts the supervisory pipeline but also severs established therapeutic relationships with clients who have built trust with their current counselor.
The Group Practice Business Model at Risk
Many Michigan group practices are built on an economic model that hires LLPCs and LLMSWs at lower compensation, then bills for their services under a fully licensed supervisor's provider number. This model depends entirely on incident-to billing. Without it, the spread between hiring cost and reimbursement shrinks to zero, or becomes negative once overhead is included. Practices that invested in growing through early-career clinicians find their financial foundation pulled away.
Sniderman's numbers illustrate the vulnerability: if a practice cannot bill for over 50% of its revenue source for a large portion of its client base, the MFT supervised experience framework itself becomes a liability. Practices may be forced to restructure as exclusively fully licensed providers, shrinking their capacity and reducing access to care.
Understanding Your Payer Mix: BCBSM, BCN, and Medicaid
Not all BCBSM plans are affected identically. The Blue Care Network (BCN) arm of BCBSM never permitted incident-to billing for limited license professionals, so BCN-heavy practices already operate without it. The new policy brings BCBSM commercial plans in line with that standard. Practices should audit their payer mix immediately to determine the precise exposure: what proportion of revenue comes from BCBSM commercial plans versus BCN, Medicare, Medicaid, or other carriers? Medicaid, for instance, may follow separate state-level rules that still allow limited license billing under supervision. A careful audit gives practice owners the numbers they need to model different staffing scenarios and explore alternative reimbursement strategies before the deadline hits.
Revenue at Risk: BCBSM's Outsized Role in Michigan Private Practices
A few key numbers underscore how heavily Michigan private practices rely on Blue Cross Blue Shield of Michigan and their limited-license workforce. With the new policy set to take effect March 1, 2027, these figures highlight why the billing change is uniquely disruptive in a state where BCBSM holds significant market share.
Facility-Based vs. Office-Based Billing and Alternative Revenue Paths
For Michigan private practices that have relied on incident-to billing for limited-license counselors, the path forward after March 2027 is a difficult choice between restructuring as a facility-based setting or building a new revenue model from scratch. Each option carries distinct financial and operational tradeoffs.
What counts as a facility-based setting under BCBSM?
BCBSM's updated policy permits incident-to billing only in facility-based settings: psychiatric hospitals, community mental health counselor jobs, federally qualified health centers (FQHCs), and outpatient psychiatric centers.1 These entities are licensed and regulated differently than office-based private practices, with requirements around clinical governance, medical records, staffing ratios, and physical space. Most independent private practices, even those with multiple clinicians, do not automatically meet these criteria. The policy explicitly ends incident-to billing in non-facility, office-based settings, which is where the majority of Michigan counseling practices operate.2
Can a private practice become an outpatient psychiatric center?
In theory, a private practice can apply to BCBSM to be recognized as an outpatient psychiatric center.3 BCBSM has directed providers to the Availity Resources portal under Billing and Claims and Medical and Reimbursement Policies for the qualification criteria. However, transforming a private practice into a facility-based entity is rarely straightforward. State licensing as an outpatient psychiatric clinic often mandates additional administrative leadership, a medical director, on-site supervision protocols, and facility upgrades that exceed typical office overhead. For a small group practice, these costs can be prohibitive. Even if a practice succeeds in restructuring, the timeline to complete the application and any required inspections before March 2027 is tight, and there is no guarantee BCBSM will approve the new designation.
Alternative reimbursement pathways to consider
Facing the loss of BCBSM commercial revenue, many practices will turn to other payers or self-pay models. Limited-license counselors in Michigan cannot bill Medicaid directly, and Medicaid fee-for-service does not recognize incident-to billing, so that avenue offers little relief. Some practice owners may pursue Employee Assistance Program (EAP) contracts, which often reimburse at a lower rate than commercial insurance but can provide a base of clients. A self-pay sliding scale model eliminates insurance dependency but requires a client population able to pay out of pocket, which may not match the existing demographic served by incident-to clinicians. It is also worth exploring whether other commercial insurers operating in Michigan still permit incident-to billing for limited-license providers in office settings, though many carriers are moving toward similar restrictions. Counselors affected by these changes, particularly those holding LPC vs LCSW credentials, should weigh how each pathway affects their long-term earning potential. For most practices, no single alternative will fully replace the volume and reimbursement levels historically delivered by BCBSM private-practice billing.
Impact on Client Access and Continuity of Care
For many Michigan clients, the upcoming BCBSM billing change forces a painful choice: pay out of pocket to continue sessions with a limited license counselor they trust, or disrupt care by transferring to a fully licensed provider, if one is even accepting new patients.
The Toll on Therapeutic Relationships
Therapeutic rapport is built over time and is a cornerstone of effective mental health treatment. Clients currently seeing a limited license counselor under BCBSM coverage often have months or years of shared history with that clinician. At WillowsEdge Counseling and Healing Arts Center, for example, 42% of clients work with limited license counselors. When these relationships are severed by billing rules, patients may experience setbacks in their recovery, loss of progress, or reluctance to start over with a stranger. For many, the emotional burden of rehashing personal struggles with a new provider can deter them from seeking help altogether.
Shortages Magnify the Impact
Michigan's mental health workforce shortage was already severe before this policy change. Statewide, 242 mental health professional shortage areas exist, covering roughly 4.2 million people, or 40 percent of the population.1 In 68 of Michigan's 83 counties, provider ratios fall below adequate levels, with rural communities disproportionately affected.2 Limited license counselors often serve as a front line in these underserved regions, practicing under supervision in clinics and private settings where fully licensed professionals are scarce. Removing their ability to bill BCBSM will shrink the pool of accessible therapists, hitting the states with highest need for counselors hardest.
Consequences for Wait Times and Access
Clients who lose coverage for their current counselor will be forced to seek care from a fully licensed provider, but those providers are in high demand. Waiting lists for an initial appointment can stretch from weeks to months, especially in rural counties or during the post-pandemic mental health surge. Some clients may delay or abandon care, risking symptom escalation, crisis episodes, or increased use of emergency services. For children, families, and individuals with complex conditions, the loss of a consistent therapeutic relationship can undo years of hard-earned stability. The policy change, while intended to ensure care from fully licensed providers, may inadvertently widen the access gap at a time when Michigan residents need mental health support more than ever.
Practical Steps for Counselors and Practice Owners Before March 2027
Understand Your Practice's BCBSM Exposure
Before you can act, you need a clear picture of your financial vulnerability. Run a revenue report by payer for the past 12 months. Separate Blue Cross Blue Shield of Michigan (BCBSM) commercial plans from Blue Care Network (BCN), Medicaid plans, and other commercial insurers. Many practices discover that BCBSM accounts for an outsized share of their income; one practice owner reported over 50% of revenue from BCBSM alone.1 Knowing your exact exposure tells you how urgently you need to diversify or restructure. If BCBSM constitutes a small slice, your path may be simpler. If it is the lifeblood of your practice, you will need more aggressive changes.
Fast-Track Full Licensure for Limited License Staff
For limited license counselors (LLPCs, LLMSWs, LLMFTs), the clock is ticking toward March 2027. If you are close to completing supervision hours, prioritize that now. Michigan typically requires 3,000 post-degree supervised hours for full licensure, but review your board's specific rules, as some hours may have been paused or modified under recent emergency orders. Contact your licensing board to confirm your progress and ask about any expedited pathways. Group supervision, co-therapy, and intensive supervision blocks can accelerate your timeline. Even if you cannot finish before the deadline, having a concrete plan demonstrates to employers and clients that you are moving toward independence, which may help you retain your position or transition to a new role.
Start Credentialing Fully Licensed Staff Now
For practice owners, BCBSM credentialing can take three to six months or longer. If you intend to shift revenue to fully licensed providers, start the credentialing process immediately. Gather all required documentation: state licenses, NPI numbers, CAQH profiles, and malpractice insurance proof. Submit applications for every fully licensed clinician on your team, even those you have not yet hired. This includes psychologists, LPCs, LMSWs, and LMFTs with unrestricted licenses. Do not wait until late 2026, as backlogs are common and you may face delays. Also, review your contracts: some BCBSM panels may be closed or have waitlists, so early submission is critical.
Diversify Revenue Streams
Reducing reliance on BCBSM is perhaps the most sustainable strategy. Consider several options: - Medicaid: Michigan's Medicaid plans often have broader inclusion of limited license clinicians under different supervision rules. Enrolling can take time but provides a stable base. - EAP Contracts: Employee Assistance Programs typically pay per session and often allow limited license providers under supervision. Reach out to local EAP networks. - Self-Pay and Sliding Scale: Develop transparent self-pay rates and a sliding-scale policy. This can attract clients who are uninsured or prefer privacy. - Telehealth Across State Lines: If you hold licenses in other states, consider offering teletherapy. Accreditation and compact privileges are expanding, so check Psychology Interjurisdictional Compact (PSYPACT) status and similar counselor compacts. Those interested in expanding to virtual services can learn more about how to become a telehealth therapist.
Communicate and Document Early
Do not surprise clients or staff. Begin informing affected clients that after March 2027, you may need to transition them to a fully licensed clinician or to an alternative payment arrangement. Frame it as proactive planning. Document these conversations in clinical notes. Also, consult a healthcare attorney to review your BCBSM contract for any transition provisions, non-compete clauses, or termination requirements. If you are considering restructuring your practice as a facility-based setting (e.g., adding psychiatric services or hospital affiliation), an attorney can help you evaluate feasibility and regulatory hurdles. Finally, keep records of all steps you take. Should BCBSM face pressure and modify the policy, your documentation may support a smoother transition back if needed.
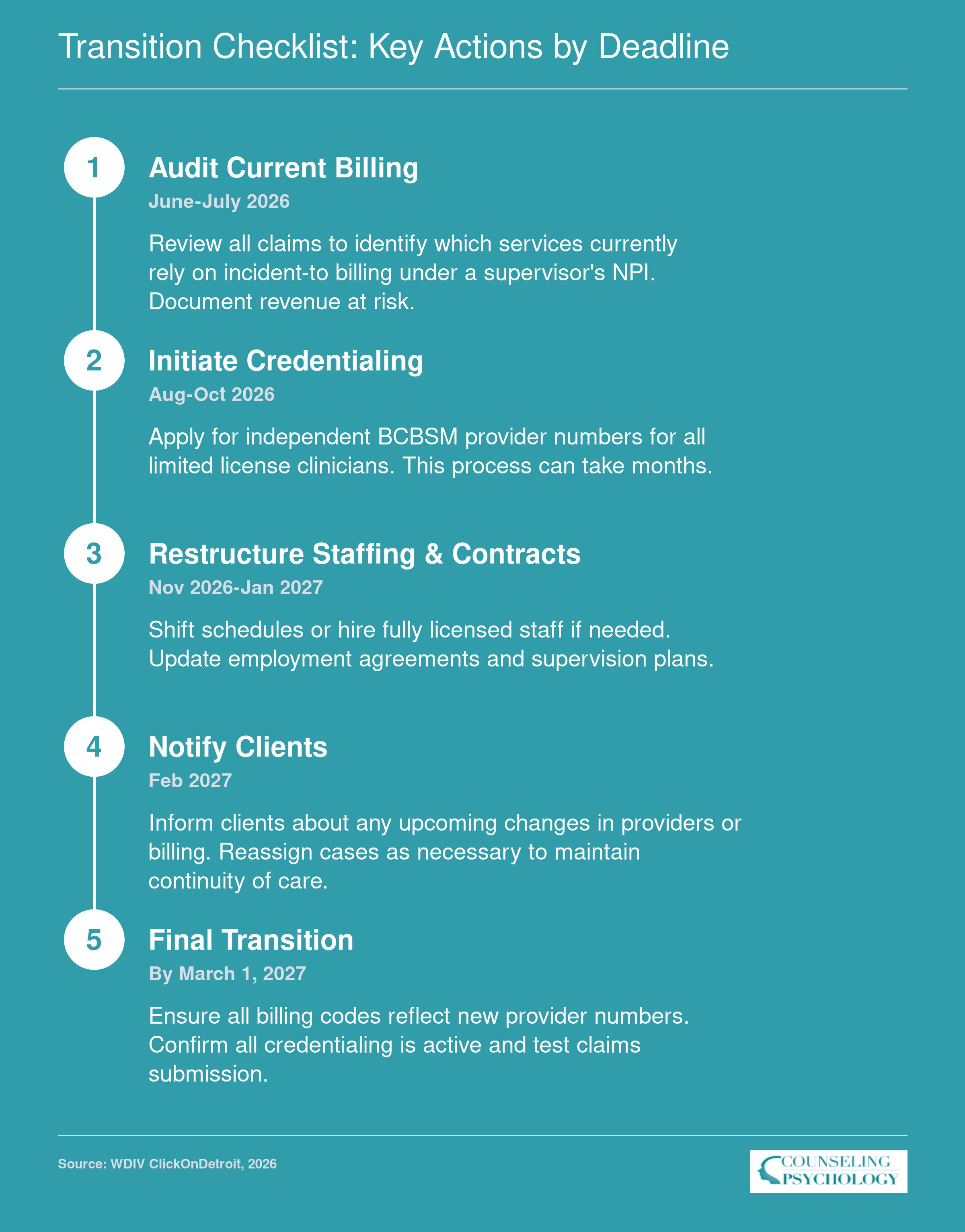
Transition Checklist: Key Actions by Deadline
To meet the March 1, 2027 deadline, private practices must take proactive steps now. Use this timeline to stay on track and avoid disruptions to care or revenue.
Advocacy Efforts and How to Get Involved
Advocacy against BCBSM's incident-to billing policy change is already organized, and the window to influence implementation is narrowing. Professional associations are mobilizing resources, coordinating legislative strategies, and calling on counselors to add their voices. Here is who is leading the effort, what actions are underway, and how you can contribute before the March 2027 deadline.
Who's Leading the Charge
The National Association of Social Workers, Michigan chapter (NASW-Michigan), has taken a central role, issuing a practice alert in 2026 and partnering with the Michigan Mental Health Counselors Association (MMHCA) to form a coalition.1 The Michigan Psychological Association (MPA) is also engaged through this joint coalition, ensuring psychologists' perspectives are included. NASW-Michigan has engaged a lobbyist and is finalizing a multi-pronged advocacy strategy that covers legal, legislative, and clinical angles. For direct inquiries, Jess Riley serves as the point person at NASW-Michigan, and the organization is actively posting updates on Facebook and Instagram.2
What's Been Done So Far
- Practice Alert: NASW-Michigan published an urgent notice detailing the policy change and its consequences for limited-license professionals, urging members to prepare and speak out.1
- Planned Survey: The association plans to survey affected clinicians to quantify the impact, data that could strengthen arguments for legislative or regulatory intervention.
- Lobbyist Engagement: A registered lobbyist is already working to educate state lawmakers about the potential harm to mental health access and the financial instability this change creates for practices.
- No Official Legislative Bill Yet: As of mid-2026, no specific bill has been introduced to counteract the BCBSM policy, and there is no identified public comment period. However, coalition partners are actively exploring legislative and regulatory avenues.1
How You Can Take Action
- Join a Professional Association: If you're not already a member of NASW-Michigan, MMHCA, or MPA, joining now strengthens the coalition's voice and provides direct access to advocacy toolkits and updates.
- Contact Your State Legislators: Reach out to your state representative and senator. Share how this policy change threatens your practice, your clients' continuity of care, and the viability of supervision models. Personalized stories carry weight.
- Monitor for Petitions and Action Alerts: Follow NASW-Michigan's social media channels and check their website for petitions, call-in days, or letter-writing campaigns. No petition is active yet, but one is likely as the survey data informs strategy.
- Write to BCBSM Provider Relations: Even without a formal comment period, sending written concerns to BCBSM's Provider Relations department documents provider opposition and may influence internal reconsideration. Outline specific operational challenges and the human cost of disrupted therapeutic relationships.
- Participate in Survey Efforts: When NASW-Michigan launches its impact survey, complete it promptly. Reliable data is essential for making a case to legislators and the insurer.
- Join Association Advocacy Committees: Many state associations have advocacy or legislative committees that coordinate grassroots efforts. Volunteering amplifies the profession's collective voice.
Media coverage has characterized the potential fallout as "devastating" for providers who rely on incident-to billing.3 Clinicians who are still working toward full licensure may also want to consider how alternative careers for counselors could serve as a contingency if practice restructuring becomes necessary. The 2027 deadline may feel distant, but policy changes of this magnitude take time to reverse. Early and sustained engagement is the most effective path toward preserving incident-to billing in private practice settings.
What This Means for Students Pursuing Counseling Careers in Michigan
The Supervision Pipeline at Risk
For aspiring counselors in Michigan, the journey to full licensure typically requires two to three years of supervised practice as a limited license professional. Many students complete these hours in private practice settings, where incident-to billing allowed them to build caseloads under a supervising clinician's provider number. With BCBSM ending this arrangement for office-based practices in March 2027, those supervision positions may shrink dramatically. Private practices that relied on limited license counselors to serve BCBSM-insured clients will likely reassess whether they can afford to keep trainees on staff if their services no longer generate revenue. This threatens the very pipeline that supplies the field with new fully licensed professionals, compounding an already well-documented mental health professionals shortage.
Where Will New Graduates Find Work?
The most immediate alternative for new graduates is employment in facility-based settings, including community mental health (CMH) agencies, psychiatric hospitals, and residential treatment centers, where incident-to billing will still be permitted. These organizations often hire limited license counselors in large numbers, but the work environment differs significantly from private practice. CMH settings typically involve higher caseloads, more administrative documentation, and less control over client scheduling. Salaries in these roles also tend to anchor at the lower end of the earnings spectrum, which may surprise graduates who expected private-practice income trajectories.
Earnings Landscape for Michigan Counselors
According to the Bureau of Labor Statistics, the median annual wage for substance abuse, behavioral disorder, and mental health counselors in Michigan was $59,530 as of the latest data, with a mean of $61,960. However, earnings vary widely: the bottom 25% made around $42,480, while the top 25% reached $74,360. Total employment in the state stood at 11,090. Students should interpret these figures carefully. Facility-based positions often align with the lower half of this range, especially during the supervised period, whereas established private practitioners with full licensure tend to earn in the upper half or beyond. The BCBSM policy change may temporarily pressure entry-level wages as more limited license professionals compete for the same hospital and CMH jobs.
Preparing for a Changing Career Path
Given the uncertainty, counseling students should be proactive. Seek clinical placements and internships in facility-based settings that are insulated from the billing change; these experiences will make you a stronger candidate for those same employers after graduation. Understanding the difference between licensure and non-licensure counseling programs is also more important than ever, since your credential level will directly affect your billing options. Discuss supervision plans early with potential supervisors to ensure your required hours can be completed without interruption if private practice billing shifts. Finally, stay informed about advocacy efforts aimed at modifying the policy: some professional organizations are pushing for carve-outs that could preserve limited license billing in certain circumstances. A flexible, informed approach to the early career phase will be essential as Michigan's mental health workforce landscape evolves.