What you’ll learn in this article…
- Research links quality supervision directly to therapist competence, client outcomes, and long-term career resilience.
- Eight recurring struggles, from evaluation anxiety to financial burden, affect new clinicians across all disciplines.
- Supervisees who build standing agendas and actively request feedback consistently report faster professional growth.
- Licensure hour requirements and supervision ratios vary significantly among counseling, social work, and MFT credentials.
Every licensed therapist in the United States must complete supervised clinical hours before practicing independently, a process that typically spans two to four years depending on discipline and state. For most early-career clinicians, those hours represent the single most formative period of professional development. They also rank among the most anxiety-producing.
The tension is real. A strong supervisory relationship sharpens clinical skills, improves client outcomes, and keeps new therapists in the field. A poor one can stall licensure timelines, erode confidence, and push talented clinicians out of the profession entirely. Research consistently links supervision quality to both therapist competence and client safety, yet many supervisees feel unprepared for the interpersonal and structural challenges the relationship introduces.
Supervision quality remains one of the strongest predictors of whether an early-career therapist thrives or burns out. The sections that follow break down the most common supervision struggles, from power imbalances and cultural dynamics to financial pressures and conflicting feedback, and offer concrete strategies to turn supervision into the growth experience it is meant to be.
Why Supervision Matters: What the Research Shows
Clinical supervision is often framed as a licensure requirement, a box to check on the path to independent practice. The evidence suggests it is doing far more work than that, shaping how competent you become, how well you connect with clients, and whether you stay in the field at all.
What Supervision Actually Changes
A 2025 systematic review and meta-analysis pooled results from 32 trials, with 13 entering the quantitative analysis.1 The findings give a nuanced picture of what supervision can and cannot deliver:
- Therapist competence: Supervision produced a small overall effect on clinician skill, but a large effect when compared against passive controls (clinicians receiving no structured oversight at all).
- Therapeutic alliance: A medium effect overall, again rising to a large effect versus passive controls. In other words, supervised clinicians build stronger working relationships with clients.
- Patient symptoms: A small and non-significant effect. Supervision improves the therapist and the alliance more reliably than it moves symptom scores directly.
A separate 2021 systematic review of supervision in mental health services reached compatible conclusions: provider competencies improved, adherence to evidence-based practice improved, and supervisees reported greater perceived support.2 Client outcome findings were mixed, mirroring the 2025 meta-analytic pattern.
Why This Matters for Early-Career Therapists
The research signal is clear on one point: structured, active supervision substantially outperforms passive or absent oversight on the things early-career clinicians most need to develop, skill and alliance. That matters because the alliance is one of the most robust predictors of client engagement, and competence is what eventually carries you through independent practice as a licensed professional counselor.
It also reframes the supervision relationship itself. If your supervisor is functioning as a passive sign-off, only initialing hours without offering case consultation, feedback on recordings, or skill-building, the evidence suggests you are getting a fraction of the benefit the format can provide. Supervision is a clinical training mechanism with measurable impact, not paperwork. Treating it that way, and expecting your supervisor to do the same, is the foundation for everything that follows in this guide.
8 Common Supervision Struggles New Therapists Face
What supervision challenges do most new therapists encounter during their first years of practice? Research and clinical training programs consistently identify eight core struggles that cut across disciplines, from vulnerability around case presentation to the practical burden of paying for required supervision hours. Recognizing these patterns can help you distinguish between normal growing pains and supervision relationships that need to change.
Vulnerability and Shame When Presenting Cases
You might find yourself editing which cases you bring to supervision, avoiding the session where you froze or said something you regret. This self-protective impulse is nearly universal: new therapists worry that revealing clinical missteps will mark them as incompetent. The result is that the cases you most need to discuss often stay hidden.
Power Imbalance and Evaluation Anxiety
When your supervisor controls your licensure hours, writes recommendation letters for psychology graduate school applications, or has formal authority over your employment, the relationship carries inherent power asymmetry. You may hesitate to disagree with feedback or advocate for your learning needs because the evaluative stakes feel too high, turning supervision into a performance rather than a learning space.
Unclear Expectations About the Supervision Process
Many supervisors assume you know what supervision should look like, but you might be left wondering whether you should bring notes, how much detail to share, or what kinds of questions are appropriate. Without explicit contracting at the start, you can spend months guessing what your supervisor actually expects from each session.
Feedback That Feels Critical Rather Than Constructive
You present a case hoping for guidance and instead hear what sounds like a list of everything you did wrong. Even well-intentioned feedback can land as harsh criticism when you are already doubting your skills, leaving you more anxious rather than more competent.
Imposter Syndrome and Self-Doubt
You passed your exams and earned your degree, but sitting with real clients can trigger intense feelings of fraudulence. Supervision can amplify imposter syndrome when you interpret every question your supervisor asks as evidence that you should not be doing this work at all.
Cultural and Identity-Based Dynamics
If your supervisor does not share your cultural background, gender identity, or lived experience, you may find yourself educating them about your clients' communities or feeling misunderstood when identity shapes your clinical choices. The growing conversation around BIPOC therapist training programs highlights how much these dynamics matter, yet they often go unaddressed in day-to-day supervision, creating subtle but persistent friction.
Time and Financial Burden of Supervision
Supervision costs range widely, from free in some agency settings to $100 or more per hour in private arrangements. When you are earning entry-level wages and need anywhere from 100 to 4,000 LMFT supervision hours depending on your license type, the financial strain is real. Finding time for supervision while managing a full caseload adds logistical pressure on top of the cost.
Conflicting Feedback from Multiple Supervisors
If you are gathering hours from more than one supervisor, you may receive contradictory advice about the same clinical situation. One supervisor encourages a directive intervention while another advocates a nondirective stance, leaving you uncertain whose guidance to follow and whether either approach is right.
Most early-career therapists experience several of these struggles simultaneously. They are not signs that you have chosen the wrong supervisor or that you are failing at clinical work. They are predictable features of a training relationship that combines learning, evaluation, and professional gatekeeping in a single role. The sections that follow explore how to navigate each challenge and when to seek a different supervision arrangement.
Ask Yourself: Is Your Supervision Working?
How Power Dynamics and Evaluation Anxiety Shape Supervision
The power dynamics in clinical supervision arise from a fundamental tension: your supervisor is both a guide to help you grow clinically and the person who decides whether you meet the requirements for licensure or continued employment. This dual role creates a backdrop of evaluation anxiety that can distort the very process meant to support your development.
The Dual Role of Supervisor: Mentor and Gatekeeper
Supervisors are expected to nurture your clinical skills while also judging your readiness to practice independently. They often sign off on licensure hours, write formal evaluations, and in many settings control your employment status. This gatekeeping function is essential to protect clients, but it places the supervisor in a position of significant authority. As a result, you may find yourself filtering what you share, trying to present a polished image of competence rather than an honest picture of your growing edges.
How This Power Imbalance Silences the Supervisee
When evaluation anxiety takes over, the very topics supervision is designed to address can become off-limits. Mistakes, countertransference reactions, and clinical uncertainty may be hidden rather than explored. Consider these common scenarios:
- A supervisee realizes they have ruptured the therapeutic alliance with a client but opts not to discuss it, hoping the supervisor will not notice. The rupture remains unaddressed and the client may leave treatment.
- A supervisor recommends a particular intervention. The supervisee genuinely believes a different, culturally adapted approach would serve the client better but stays silent to avoid appearing argumentative or disrespectful.
- A therapist feels completely overwhelmed by their caseload, working late and cutting corners on documentation. They do not mention it in supervision, fearing it will reflect poorly on their time management or commitment, and the pattern intensifies.
In each case, the power differential prevents the open dialogue that leads to better client care and your professional growth.
Practical Strategies to Manage the Power Differential
You can take steps to reduce the impact of evaluation anxiety. One effective approach is to initiate a conversation early about how evaluations work. Ask your supervisor what specific criteria they use, how often they give feedback, and what confidentiality boundaries exist. Knowing the rules of the game can lower your anxiety and make the process feel less arbitrary.
Another powerful strategy is to request separate formative and summative feedback sessions. Formative feedback is ongoing, developmental, and meant to help you improve; summative feedback is the final evaluation. Having dedicated time for case discussion that is explicitly not evaluative can create a safe space to explore your vulnerabilities without the fear of immediate career consequences. For those navigating the MFT track specifically, understanding mft supervision requirements ahead of time can further reduce uncertainty about what your supervisor expects and when key milestones need to be met.
Related Articles
Navigating Cultural and Identity-Based Challenges in Supervision
Supervision carries an inherent tension for many early-career clinicians: the relationship is designed to foster growth, yet the power imbalance within it can silence the very perspectives that make care culturally effective. For supervisees from marginalized backgrounds, this tension is often sharpest.
When Identity Becomes a Liability Instead of an Asset
Research on multicultural supervision consistently documents a troubling pattern: supervisees from BIPOC, LGBTQ+, and first-generation professional backgrounds are more likely to experience microaggressions within supervision than their peers.1 These are not always overt. They show up as color-blindness ("I treat all my clients the same"), minimization of cultural context, exoticization of a supervisee's background, or what researchers describe as overburdening, where a clinician of color is repeatedly assigned or consulted on every client from a similar background as though they represent an entire community.
The consequences are measurable. Studies link these supervisory microaggressions to poorer working alliances, reduced self-disclosure, lower self-efficacy, and elevated burnout risk.1 When supervisees fear negative evaluation or retaliation, they stop bringing the clinical material that matters most.4
Three Scenarios Worth Naming
Consider these situations, each of which practitioners commonly report:
- The BIPOC supervisee whose culturally grounded intervention, perhaps drawing on familismo or community-centered healing, is questioned as "non-evidence-based" without the supervisor engaging with the underlying clinical rationale.
- The LGBTQ+ clinician whose identity is framed by a supervisor as a potential countertransference risk rather than a source of informed empathy, effectively positioning lived experience as a liability.
- The first-generation professional who lacks the unspoken cultural capital of graduate training norms, never quite sure whether to push back or defer, and finding that no one has made those unwritten rules explicit.
In each case, the problem is not the supervisee. It is a supervision relationship that lacks cultural humility.
What Culturally Responsive Supervision Actually Looks Like
The APA's guidelines for clinical supervision, adopted in 2014 and organized across seven domains, explicitly require that evaluation account for cultural context and that supervisors demonstrate diversity competence.2 A well-structured supervision contract should address cultural expectations from the outset, not as an afterthought.
Culturally responsive supervision models, including relational-cultural, feminist-informed, and cultural humility-based approaches, share a common thread: the supervisor actively examines their own cultural position rather than treating the supervisee's identity as the variable that needs managing.1 Research on supervisory relationships finds that supervisor cultural humility is inversely related to supervisee nondisclosure, and that this relationship is mediated by the quality of the working alliance.3 In plain terms: when supervisors lead with humility, supervisees share more, and outcomes improve. For clinicians interested in deepening this competency, exploring a path as a multicultural counselor offers structured training in these frameworks.
How to Raise Cultural Concerns in Supervision
If you are navigating these dynamics, consider the following approaches:
- Name it early: Raise cultural and identity-related expectations during your first supervision session. Ask how your supervisor approaches multicultural case conceptualization.
- Use the contract: A supervision contract is a legitimate place to document how cultural concerns will be addressed. Propose including it if your supervisor has not.
- Document patterns: If microaggressions are recurring, keep a factual record with dates and context. This matters if a formal complaint becomes necessary.
- Know the threshold: Cultural incompetence becomes an ethical issue when it compromises client care, silences clinically relevant information, or constitutes discriminatory treatment. ACA and APA ethics codes both speak to this.
Seeking peer consultation or working with a secondary supervisor who shares or affirms your cultural context is not a workaround. It is sound professional practice.
Key Insight: Supervision Should Be a Two-Way Relationship
The most productive supervision happens when you show up as an active partner, not a passive trainee. That means bringing specific cases, naming your uncertainties, requesting the feedback you need, and pushing back respectfully when something does not fit. Your supervisor brings expertise, but you bring the clinical material and the questions that shape what gets learned.
What to Do If Supervision Is Harmful or Unethical
Professional ethics codes explicitly protect supervisees from harm, yet many early-career therapists remain silent when supervision crosses ethical lines. Fear of retaliation, delayed licensure, or professional blacklisting keeps harmful dynamics hidden.1 Understanding your rights and the formal escalation pathways available can empower you to address serious supervision failures without derailing your career.
Recognizing Harmful Supervision
Harmful supervision takes many forms, all of which violate professional standards. Boundary violations include romantic or sexual advances, requests to meet outside professional settings without clinical justification, or sharing personal problems that burden the supervisee. Exploitation occurs when supervisors assign excessive administrative work unrelated to clinical development, require unpaid labor beyond agreed hours, or claim credit for supervisee scholarship or clinical contributions. Discrimination based on race, gender, sexual orientation, religion, or disability violates federal law and every major mental health profession's ethics code. Failure to provide adequate oversight, such as canceling supervision sessions repeatedly, offering no meaningful feedback on clinical work, or signing off on hours without reviewing case material, constitutes professional negligence. Retaliation for disagreement, including hostile responses to supervisee questions or threats to withhold required hours when a supervisee raises concerns, creates a coercive environment. Sexual harassment, whether through explicit propositions, repeated comments about appearance, or sharing sexual material, is both an ethical violation and illegal workplace conduct.
The Stepwise Escalation Guide
When supervision becomes harmful, follow a clear escalation process. First, document specific incidents with dates, locations, direct quotes when possible, and names of any witnesses. Keep these records in a secure personal location separate from your workplace. Second, if you feel physically and professionally safe, attempt a direct conversation with your supervisor using neutral language focused on observable behavior and your needs. Frame the discussion around professional standards rather than personal grievances. Third, consult a trusted colleague, mentor outside your direct chain of supervision, or a faculty advisor who can offer perspective and guidance.1 Fourth, report internally to your training director, agency clinical director, or human resources department, providing your written documentation. Fifth, file a formal complaint with the relevant state licensing board that regulates your supervisor's credential, or with your professional association. The American Psychological Association, American Counseling Association, National Association of Social Workers, and American Association for Marriage and Family Therapy all maintain ethics committees that investigate member conduct. Sixth, if the situation remains unresolved or unsafe, seek a new supervisor. Your licensing board can often provide guidance on transferring accrued hours and finding alternative supervision arrangements.
Ethical Codes That Protect You
Every major mental health profession's ethics code includes explicit supervisor responsibilities. The ACA Code of Ethics devotes Section F to supervision, training, and teaching, mandating that supervisors maintain appropriate boundaries, provide competent oversight, and avoid exploiting students or supervisees.1 The APA Ethical Principles address supervision across 12 sections, emphasizing informed consent, competence boundaries, and prohibition of sexual relationships with supervisees. NASW standards frame supervision as a formal professional responsibility requiring clear expectations, regular feedback, and cultural responsiveness. The AAMFT Code of Ethics requires supervisors to maintain competence in supervision itself, avoid exploitation, and uphold strict boundaries. These codes exist to protect you, not to shield problematic supervisors. Marriage and family therapists navigating the specifics of supervision of MFT trainees should familiarize themselves with both their state requirements and the AAMFT standards that govern supervisor conduct.
Addressing the Fear of Reporting
The most common barrier to reporting harmful supervision is fear that doing so will delay licensure, damage professional reputation, or end a career before it begins. These fears are understandable but often overstated. State licensing boards exist to protect the public and the profession, which includes protecting supervisees from harm. Most boards maintain confidentiality during investigations and prohibit supervisor retaliation. Professional associations investigate complaints separately from state licensure processes, meaning an association ethics finding does not automatically trigger license sanctions.1 If you must change supervisors mid-stream, licensing boards routinely approve hour transfers when supervisee safety or professional development is at stake. Documenting the process, seeking consultation before acting, and following established grievance procedures actually protects your licensure pathway by creating a clear record of your professionalism. Silence, by contrast, allows harmful patterns to continue and may implicate you if a supervisor's misconduct later comes to light through other channels. Your obligation to future supervisees and clients justifies the risk of speaking up.
Practical Strategies to Get More from Your Supervision
The supervisees who grow fastest are the ones who treat supervision as a skill to practice, not a requirement to endure.
Build a Standing Agenda
Walking into supervision without a plan is one of the most common ways early-career therapists leave value on the table. A simple four-part agenda, brought to every session, keeps the work focused and signals to your supervisor that you take the relationship seriously.
- Case update: Briefly flag any clients whose presentations have shifted, escalated, or raised new clinical questions since your last meeting.
- Skill I want to develop: Name one specific competency you are working on this week, whether that is tolerating silence, pacing a trauma narrative, or sharpening your case conceptualization.
- Ethics or boundary question: Even a small dilemma worth thinking through out loud. These conversations build ethical muscle over time.
- Feedback request: Ask for one concrete piece of feedback on something you did in session. Vague requests get vague answers.
Sending this agenda by email the day before supervision serves a dual purpose: it helps your supervisor prepare, and it creates a paper trail of your professional growth.
Scripts for Difficult Conversations
Asking for what you need can feel uncomfortable when there is an evaluative dimension to the relationship. Having language ready reduces the friction.
To ask for more structured feedback: "I find I retain feedback better when it is specific. Would you be willing to tell me one thing I did effectively and one thing to work on after we discuss a case?"
To raise a clinical disagreement: "I want to think through this with you because my instinct was pulling in a different direction. Can I share my reasoning so we can figure out where we diverge?"
To request focus on a competency area: "I have been feeling less confident with clients presenting grief and loss. Could we dedicate part of our next few sessions to building that up?"
None of these scripts are confrontational. They are direct, which is exactly what good supervision asks of you.
Use Deliberate Practice Between Sessions
Recording sessions with client consent and reviewing them before supervision is one of the highest-yield activities available to new therapists. Watching yourself on video surfaces habits you cannot catch in the moment: filler language, rushed reflections, missed nonverbal cues. Bring specific timestamps to supervision rather than a general sense that something felt off.
Tracking your development over time matters too. A simple running document, one entry per supervision session noting what you worked on and what shifted, creates the longitudinal evidence you will need for licensure documentation and for your own confidence.
Managing Up When Your Supervisor Is Less Engaged
Not every supervisory relationship is well-matched, and not every supervisor is equally invested. If yours tends toward the passive end, there are concrete ways to shape the relationship without overstepping.
Propose a supervision contract at the outset or at any natural reset point. This document can outline your learning goals, preferred feedback style, and expectations for documentation. Framing it as a mutual agreement rather than a demand usually lands well. If you are pursuing marriage and family therapy licensure, our guide on MFT program mentorship walks through the structure of these agreements in more detail.
Request written evaluations at regular intervals, such as every three months, and frame the request around your licensure goals. Written evaluations create accountability for both parties and give you documented evidence of competency growth that will matter when you apply for licensure.
The underlying principle across all of these strategies is the same: supervision works best when you treat it as an active collaboration rather than something that happens to you.
How Supervision Requirements and Struggles Differ by Discipline
Supervision is required across every clinical license, but the volume of hours, the ratio of supervision to practice, and the type of work that counts toward your hours vary significantly by discipline. Understanding what your specific license demands, and where the friction points tend to emerge, helps you plan realistically and advocate for yourself when supervision falls short.
Licensed Professional Counselors (LPC/LCPC)
Most states require 2,000 to 4,000 total supervised hours for LPC or LCPC licensure, with a common ratio of one hour of supervision per 20 to 40 clinical hours.12 Supervisors are typically licensed counselors, though many states also accept LCSWs, LMFTs, psychologists, or psychiatrists.3 A frequent struggle here is the direct-versus-indirect hour split: many states require at least 50% direct client contact, and a few count only direct hours, which can extend your timeline if your agency loads you with paperwork, case management, or no-shows.4 If you are still exploring the path to becoming a licensed professional counselor, understanding these hour requirements early is critical.
Licensed Marriage and Family Therapists (LMFT)
LMFT candidates generally need around 3,000 supervised hours, with at least one supervision hour per 5 to 10 direct client hours early in training, or a weekly minimum.5 Supervisors must usually hold an AAMFT-approved supervisor credential or a state equivalent.6 The defining requirement is relational hours: many boards expect 1,000 or more hours working with couples and families, not individuals.5 New LMFTs in agencies that primarily serve individual clients often scramble to find relational caseload, which is a common bottleneck.
Licensed Clinical Social Workers (LCSW)
LCSW requirements typically total 3,000 hours, with at least one weekly supervision hour or one hour per 30 to 40 hours of practice.56 Supervisors must be LCSWs, though some states allow a psychologist or psychiatrist to cover a portion.6 Like LPCs, social workers often face a 50% direct contact rule, and ASWB documentation standards are detailed: expect to log dates, hours, modality, and supervisor signatures meticulously.
Licensed Psychologists
The psychology path is the longest. Doctoral candidates complete a 2,000-hour APA-accredited internship plus a postdoctoral year of 1,500 to 2,000 hours, with two or more supervision hours per week typical during both.7 Supervisors must be licensed psychologists with appropriate post-licensure experience.7 The core challenge is breadth: boards expect demonstrated competency across therapy, assessment, consultation, and often research, which means your supervision should span all of these, not just psychotherapy.
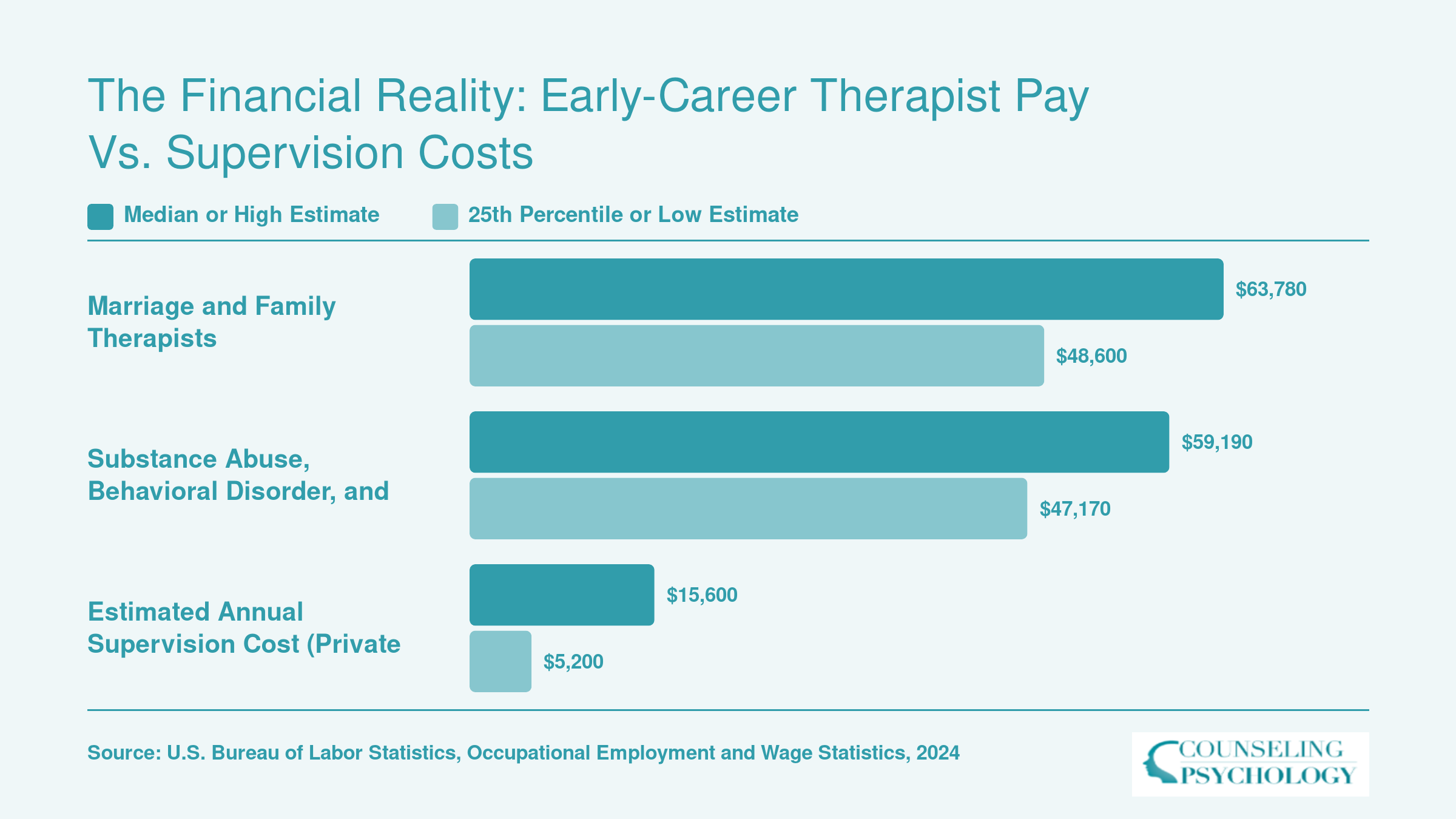
The Financial Reality: Early-Career Therapist Pay vs. Supervision Costs
Supervision is essential for licensure, but the financial math can be sobering. Marriage and family therapists earn a median salary of $63,780, while substance abuse, behavioral disorder, and mental health counselors earn a median of $59,190. When you layer private-pay supervision fees on top of those starting-range salaries, the out-of-pocket burden becomes clear. Many agency positions bundle supervision into the job but offset that benefit with lower base pay, while clinicians headed for private practice often absorb the full cost themselves, typically $100 to $200 per session, one to two hours per week, for two to three years.
Choosing a Clinical Supervisor: What to Look For
Selecting your first clinical supervisor means balancing multiple priorities: finding someone whose theoretical framework meshes with yours, whose availability fits your schedule, and whose supervisory style supports your learning, all while navigating the constraints of your setting and budget. Whether you are assigned a supervisor through your agency or hiring one independently for licensure hours, the quality of that relationship will directly shape your clinical development and your emotional experience of early practice.
Five Criteria for Evaluating a Potential Supervisor
Before committing to a supervisor, assess these core dimensions:
- Clinical orientation alignment: If you practice from a trauma-informed, attachment-based lens and your supervisor leans heavily on CBT protocols, your case conceptualizations may clash repeatedly. Look for supervisors whose theoretical orientation complements or enriches your own.
- Supervisory style: Some supervisors are directive, offering concrete suggestions and corrective feedback quickly. Others take a collaborative, strengths-based approach, asking reflective questions and encouraging you to generate your own solutions. Neither is inherently better, but mismatched styles can create frustration on both sides.
- Cultural competence: A supervisor should be able to discuss race, ethnicity, gender, sexuality, and other identity dimensions openly and without defensiveness. Ask yourself whether this person can help you navigate cultural dynamics in your cases and whether they acknowledge their own positionality.
- Availability and responsiveness: Will your supervisor be reachable between sessions if you face a crisis or ethical dilemma? How quickly do they typically respond to emails or texts? Clarify expectations upfront.
- Willingness to discuss the supervisory relationship: The best supervisors model the same transparency and repair they expect you to practice with clients. They welcome meta-conversations about what is and is not working in supervision.
Questions to Ask Before You Commit
Treat your initial meeting as a two-way interview. Consider asking:
- How do you handle disagreements or moments when we see a case differently?
- What does a typical supervision session look like with you?
- How do you approach cultural differences between us or between me and my clients?
- What is your philosophy on giving corrective feedback, and how soon do you typically offer it?
These questions reveal whether a supervisor is reflective, whether they have a coherent supervisory framework, and whether they can articulate their process in a way that makes sense to you.
Agency-Assigned vs. Private-Pay Supervisors
If your employer assigns your supervisor, you have less control over fit but more structure and often no out-of-pocket cost. In these situations, managing up becomes essential: set your own agenda for sessions, ask for what you need, and document your hours carefully. If the fit is poor, explore whether your agency allows supervisor changes or whether you can supplement with outside consultation.
Private-pay supervisors offer more choice but require financial investment, typically between seventy-five and two hundred dollars per session depending on region and credentials. The stakes for fit are higher because you are funding the relationship directly. Interview multiple candidates and trust your gut about rapport and safety. If you are pursuing marriage and family therapy licensure, understanding MFT supervision requirements before selecting a private-pay supervisor can help you avoid costly missteps.
Switching Supervisors Mid-Licensure
Switching supervisors is possible and sometimes necessary for your professional development or emotional health. To do so without burning bridges:
- Give honest, tactful feedback about why the relationship is not meeting your needs.
- Provide reasonable notice (two to four weeks if possible) so your supervisor can adjust their schedule.
- Request a final meeting to review outstanding hours, sign necessary documentation, and express gratitude for what you did gain.
- If the supervision was harmful or unethical, you are not obligated to provide extensive explanation. A brief, professional notice is sufficient, and you may need to consult your licensing board or a trusted mentor about next steps.
Your supervisor is not your therapist, but the relationship should still be marked by mutual respect, psychological safety, and a shared commitment to your growth.