What you’ll learn in this article…
- Outpatient substance abuse counselors carry an average caseload of 26 clients, rising past 130 in community settings.
- Documentation and administrative tasks consume roughly 40 percent of a typical counselor's workday.
- Inpatient, outpatient, and telehealth settings differ sharply in shift length, crisis exposure, and session frequency.
- Clinical supervision is the most consistently cited protective factor against counselor burnout and turnover.
Substance abuse counselors work within a rhythm that is both predictable and impossible to script. A typical outpatient counselor sees four to six individual or group sessions per day, spends two to three hours on case notes and treatment plans, and participates in at least one multidisciplinary team meeting or supervision session per week. Yet within that framework, crisis calls, urgent care walk-ins, and relapse episodes regularly upend the schedule.
The structure is real. The rhythm is learnable. But the human variability ensures that no two Tuesdays will ever look exactly alike.
This article walks through the mechanics of the workday: hour-by-hour schedules, setting-specific differences between inpatient residential, outpatient clinic, and telehealth roles, average caseloads by environment, and how the job evolves as you advance from entry-level CADC to senior clinical supervisor. Each section is designed to help anyone considering a graduate certificate in addictions counseling or master's program in addiction counseling understand what the daily work actually demands, not just what the job description promises.
What a Substance Abuse Counselor Actually Does Each Day
A substance abuse counselor's daily work is a mix of face-to-face client sessions, group facilitation, crisis response, and a substantial amount of documentation. If you picture the job as eight hours of deep therapeutic conversation, the reality will surprise you: administrative tasks like updating treatment plans, writing progress notes, and coordinating with insurance companies consume nearly as much time as clinical contact, and sometimes more.
The Core Functions That Fill Your Hours
Addiction counseling is formally organized around 12 Core Functions, a framework recognized by credentialing bodies and training programs nationwide. Not all 12 show up every single day, but several are constant fixtures. Assessment, treatment planning, and counseling (both individual and group) form the backbone of clinical work. Case management and referral round out the picture, since counselors regularly connect clients to housing services, psychiatric care, vocational rehabilitation programs, or mutual-aid groups. Crisis intervention may not be scheduled, but it happens often enough that experienced counselors treat it as a standing part of the workday rather than an exception.
Screening, intake, and orientation tend to cluster around new admissions. Report and recordkeeping, on the other hand, follows you home in spirit if not in practice. Consultation, whether with supervisors, physicians, or probation officers, is woven into team meetings and quick hallway check-ins throughout the week.
Clinical Tasks vs. Administrative Tasks
It helps to think of your day in two broad categories:
- Clinical contact: Individual counseling sessions, group therapy facilitation, psychoeducational classes, crisis de-escalation, and family sessions.
- Administrative work: Electronic health record (EHR) documentation, treatment plan updates, insurance authorization calls, discharge summaries, and interdisciplinary staffing notes.
National data on behavioral health counselors indicates that direct client contact accounts for roughly 30 to 45 percent of a typical workweek, translating to about 12 to 18 hours.1 Documentation and other administrative duties fill 40 to 60 percent of working hours, or approximately 16 to 24 hours per week.1 That ratio can feel lopsided, and it is a consistent source of frustration across the field. The shift toward electronic records has added structure but also volume: a 2024 federal report from the Office of the National Coordinator for Health IT found that 68 percent of substance use and mental health treatment facilities used EHR systems exclusively, with another 25 percent operating in a hybrid paper-and-digital model.2 More digital documentation means more time at a keyboard after sessions end.
Skills You Practice Every Day
The clinical techniques you deploy daily go well beyond "talk therapy" in a generic sense. Motivational interviewing is a staple, particularly with clients who are ambivalent about change or early in recovery. Active listening underpins every interaction, from a routine check-in to a high-stakes crisis call. Cultural competency is not an elective skill; counselors work with clients across a wide range of racial, ethnic, socioeconomic, and linguistic backgrounds, and the ability to adapt your approach matters in every session. If you want to deepen this competency, formal multicultural counseling training can be a worthwhile investment.
You will also rely on de-escalation techniques, boundary-setting, and documentation accuracy as daily competencies. The counselors who thrive long-term tend to be the ones who treat both the clinical and administrative halves of their role as equally important, since a well-written treatment plan protects clients just as much as a well-run group session does. For a broader look at how these responsibilities compare across the profession, see our overview of a day in the life of a mental health counselor.
Hour-By-Hour: A Typical Workday Schedule
While no two days are identical, substance abuse counselors tend to follow a structured daily rhythm that balances direct client contact with documentation, team coordination, and professional development. The schedule below reflects a common outpatient setting with standard business hours, though shifts can vary significantly in residential or crisis environments.
| Time Block | Activity | Notes |
|---|---|---|
| 7:30 a.m. to 8:00 a.m. | Arrive and review schedule | Check voicemails, review client charts, confirm appointment attendance, and flag any crisis follow-ups from the previous day. |
| 8:00 a.m. to 9:00 a.m. | Facilitate morning group therapy session | Common topics include relapse prevention, coping skills, or 12-step psychoeducation. Groups typically include 8 to 12 participants. |
| 9:00 a.m. to 10:30 a.m. | Individual counseling sessions (2 back-to-back) | Sessions run 45 to 50 minutes each, covering treatment plan goals, motivational interviewing, or crisis stabilization as needed. |
| 10:30 a.m. to 11:00 a.m. | Clinical documentation | Complete session progress notes, update treatment plans, and log required data for state or federal reporting. |
| 11:00 a.m. to 12:00 p.m. | Intake assessment or biopsychosocial interview | New client evaluations include substance use history, mental health screening, and determination of appropriate level of care. |
| 12:00 p.m. to 12:45 p.m. | Lunch and informal peer consultation | Many counselors use part of this break to decompress or briefly consult colleagues about challenging cases. |
| 12:45 p.m. to 2:15 p.m. | Individual counseling sessions (2 back-to-back) | Afternoon sessions may include family members or focus on discharge planning for clients nearing the end of treatment. |
| 2:15 p.m. to 3:00 p.m. | Multidisciplinary team meeting or clinical supervision | Collaborate with psychiatrists, social workers, case managers, and supervisors to coordinate care and discuss high-risk cases. |
| 3:00 p.m. to 4:00 p.m. | Facilitate afternoon group session | Process-oriented or skills-based groups, such as cognitive behavioral therapy for substance use or emotional regulation. |
| 4:00 p.m. to 4:30 p.m. | Documentation, phone calls, and care coordination | Finalize remaining notes, return calls to referral sources or probation officers, and prepare files for the next day. |
| 4:30 p.m. to 5:00 p.m. | Self-care and end-of-day wrap-up | Review the next day's schedule, complete any outstanding administrative tasks, and practice brief stress-reduction routines before leaving. |
Questions to Ask Yourself
Inpatient Vs. Outpatient Vs. Telehealth: How the Day Differs
The setting where you practice shapes nearly every aspect of your workday, from shift length and crisis exposure to the kinds of clients you serve. Here is a side-by-side look at how inpatient residential, outpatient clinic, and telehealth roles compare across the dimensions that matter most to working counselors.
| Dimension | Inpatient Residential | Outpatient Clinic | Telehealth |
|---|---|---|---|
| Shift structure | 8 to 12 hour shifts in a 24/7 program; rotating days, evenings, and weekends are common | Standard clinic hours; OP clients attend 1 to 2 days per week, IOP clients 3 to 5 days, PHP clients 5 to 7 days | Flexible scheduling that often includes evenings and weekends; sessions delivered from home or a clinic office |
| Typical session length | Groups run 60 to 90 minutes; individual sessions run 30 to 60 minutes | Individual sessions run 45 to 60 minutes; groups run 60 to 90 minutes; IOP blocks last 3 to 4 hours; PHP blocks last 4 to 6 hours per day | Individual sessions run 30 to 60 minutes; groups run 60 to 90 minutes; short check-ins are common between scheduled appointments |
| Daily session mix | Multiple group sessions each day, 1 to 2 individual sessions per week per client, plus family sessions | OP: 1 to 2 groups per week with weekly or biweekly individual sessions; IOP: group sessions 3 to 5 days per week with individual sessions layered in | Mix of individual and group sessions; high-frequency brief check-ins; medication-assisted treatment (MAT) visits often integrated |
| Crisis frequency | Highest of all settings; withdrawal episodes, self-harm risk, and behavioral crises occur regularly throughout shifts | Moderate overall, though higher in IOP and PHP tracks; crises during off-hours are typically routed to the emergency department | Comparable to outpatient in acuity level; counselors follow structured remote safety protocols and coordinate with local emergency resources when needed |
| Documentation load | Heavy volume of notes (admission, daily progress, group, treatment plans, discharge summaries), usually completed in dedicated blocks during or after shift | High-frequency note writing tied to every client contact; strong emphasis on utilization review and insurance authorization | High and tightly structured; each note must record the modality used, informed consent for telehealth, technology platform details, and the physical location of both counselor and client |
| Client population | Clients with the most severe substance use disorders; many face unstable housing, limited social support, or legal system involvement | Less acute clients who are able to live at home; a mix of employed and unemployed individuals stepping down from higher levels of care | Broadest geographic reach, serving rural residents, people without reliable transportation, working caregivers, and clients who prefer the privacy of a remote setting |
| Pace and predictability | Fast-paced with frequent interruptions; the milieu environment means you are 'on' throughout the shift | More predictable rhythm built around a fixed appointment schedule, though IOP and PHP days can feel intensive | Counselor has more control over pacing; screen fatigue and the need for strong self-directed time management are the main challenges |
Caseload, Session Counts, and Documentation Time
Outpatient substance abuse counselors in the U.S. carry an average caseload of 26 clients, a figure that can climb to 130 or more in community mental health settings.1 These numbers directly shape daily session loads, paperwork demands, and long-term job sustainability.
Caseload by Setting
Caseload varies dramatically by treatment environment. In outpatient clinics, the average counselor is responsible for 26 clients, though programs with accreditations like CARF often report about 6 fewer clients per counselor.1 Inpatient and residential programs typically assign lower caseloads of 15 to 30 patients because counselors provide daily therapeutic contact. Community mental health counselor roles present the widest range, with some professionals managing combined active and maintenance caseloads of 60 to 130 individuals, a workload that frequently includes intensive case management duties.2
Daily Session Counts
In a typical full-time outpatient schedule, a counselor facilitates 5 to 8 individual or group counseling sessions each day. Clients receive more than 5.5 hours of counseling weekly plus about 50 minutes of case management, so session frequency adds up quickly.1 Inpatient counselors often conduct fewer daily sessions because each interaction runs longer and integrates milieu therapy, family meetings, and treatment planning. Group-based intensive outpatient programs (IOPs) may condense 9 or more hours of therapy into a few weekday blocks, raising the daily contact count.
Documentation and Compliance: The Hidden Second Job
Progress notes, treatment plans, and insurance pre-authorizations consume a significant share of a counselor's day. A single progress note can take 5 to 15 minutes to complete. With 5 to 8 sessions, that alone adds an hour or more of documentation. Factor in electronic health record (EHR) requirements, utilization reviews, and pre-authorization calls for continuing care, and the administrative side continues long after the last client leaves. Counselors in community settings often handle additional paperwork for housing, court, or social services referrals, sharply increasing non-clinical hours.
Caseload and Burnout: A Critical Connection
High caseloads are a primary driver of burnout in addictions counseling. When session counts and paperwork overwhelm a counselor's capacity to build genuine therapeutic relationships, job satisfaction drops and turnover rises. Setting realistic caseload expectations and protecting documentation time are not just efficiency measures but essential components of a sustainable career in counseling.
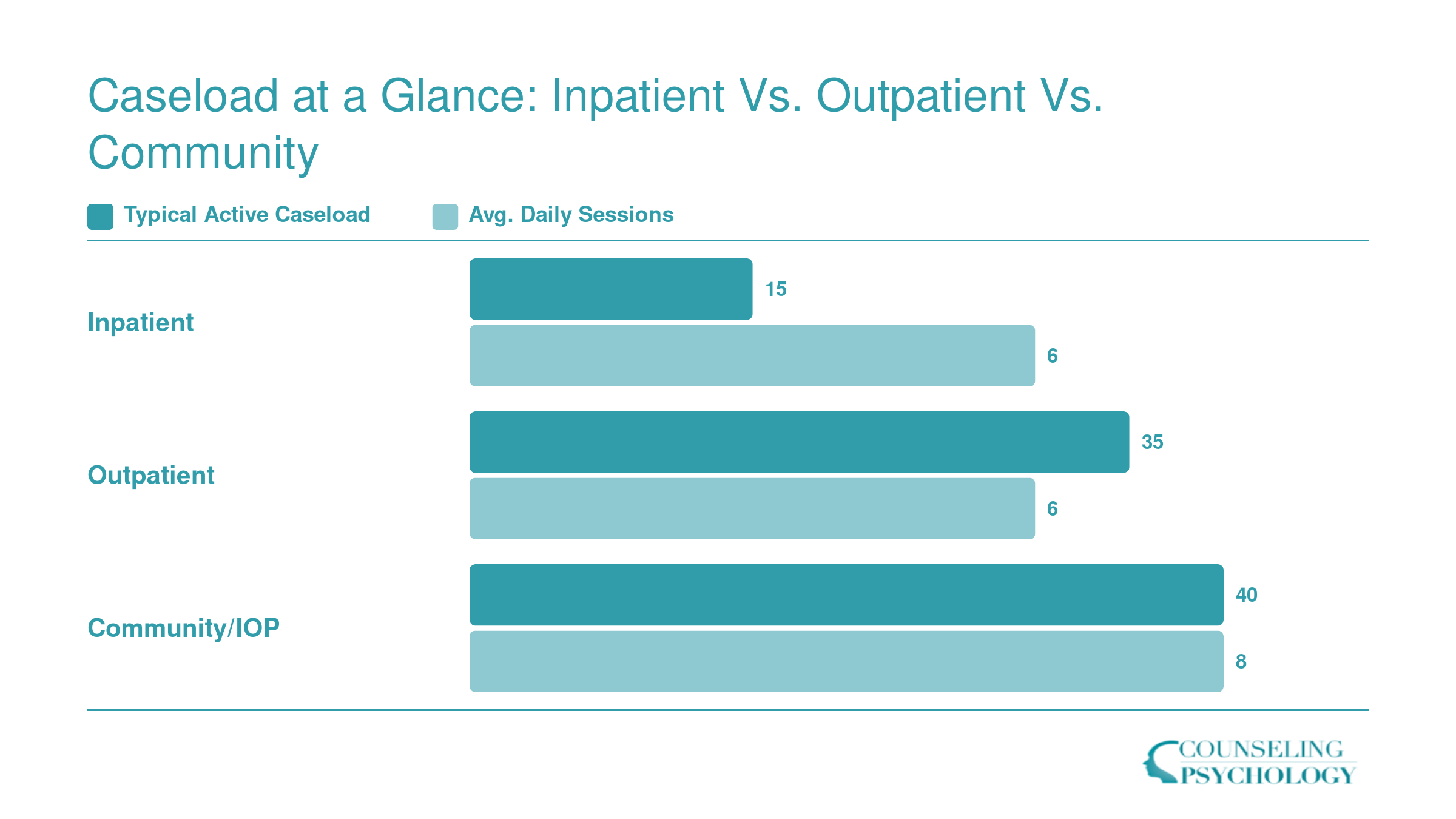
Caseload at a Glance: Inpatient Vs. Outpatient Vs. Community
Caseload size and daily session counts vary significantly depending on your work setting. Inpatient counselors typically carry smaller active caseloads but see clients more frequently throughout the day, while outpatient and community or IOP counselors manage larger rosters with fewer face-to-face contacts per day.
Team Meetings, Supervision, and Multidisciplinary Collaboration
Substance abuse counseling has become increasingly team-based, with solo practice the exception rather than the rule across inpatient, outpatient, and community settings alike.
Clinical Supervision: The Cadence and the Stakes
For pre-licensed counselors holding credentials like a CADC-I or an associate-level license, supervision is not optional background noise. It is a structured, required part of the job. The typical rhythm is weekly individual supervision with a clinical supervisor, supplemented by biweekly group supervision sessions. Hours logged in this structure count directly toward licensure accrual, which means missing them has real consequences for a counselor's timeline to independent practice. Understanding how supervision hours accumulate across disciplines can give you a clearer picture of what to expect.
Even after licensure, supervision does not disappear entirely. Licensed counselors often participate in peer consultation or group case review on a biweekly or monthly basis, which sustains clinical quality and reduces the isolation that can build quietly in this field. The supervision load, and the purpose behind it, shifts significantly as counselors advance. That progression is worth understanding before you picture your long-term schedule.
Multidisciplinary Team Meetings
On any given week, a substance abuse counselor may sit in on one or more multidisciplinary team meetings. The cast in the room typically includes a psychiatrist or psychiatric nurse practitioner, a social worker, a case manager, and a floor or intake nurse in residential settings. Telehealth and outpatient programs often hold these meetings virtually, but the agenda is similar regardless of format.
What gets discussed: treatment plan reviews, discharge planning, medication coordination, and flags for clients showing signs of crisis or stalled progress. The counselor's role is not passive. They are expected to bring a clinical read on each client, advocate for treatment adjustments, and follow up on action items before the next meeting.
Collaboration as a Core Competency
Listing "strong collaboration skills" on a counselor resume is common. Living it out across a 40-hour week is something different. Substance abuse counselors negotiate with case managers over housing barriers, consult with nurses about withdrawal protocols, and coordinate with court liaisons when clients have legal mandates attached to their treatment. These interactions happen in hallways, over secure messaging platforms, and in formal meeting rooms.
Counselors who struggle with communication across professional disciplines often find the work harder than they anticipated. Those who thrive in cross-functional environments tend to find it one of the most energizing parts of the role.
The Emotional Reality: Common Stressors, Rewards, and Self-Care
Substance abuse counseling carries a well-documented emotional toll, with turnover rates in residential treatment settings reaching 62% in Michigan alone1 and a projected national shortage of 114,000 addiction counselors by 2037.2 The work is deeply human, but the accumulated weight of secondary traumatic stress, administrative pressure, and client setbacks can push even the most dedicated professionals toward compassion fatigue.3
The Stressors That Wear Counselors Down
The daily stressors cluster around a few relentless themes. Client relapse tops the list: after months of building a therapeutic alliance and witnessing hard-won progress, a return to active use can feel like a personal failure, even when counselors intellectually understand the chronic nature of addiction. High caseloads magnify the strain, with many counselors managing far more clients than the recommended threshold, leaving little time to process one crisis before the next arrives. Secondary traumatic stress accumulates as counselors absorb detailed histories of abuse, overdose, and loss.3 The administrative load adds another layer: prior authorizations, treatment plan documentation, and insurance billing can consume hours that feel stolen from direct care. While every substance use disorder presents unique challenges, many counselors point to polysubstance use and opioid use disorder as particularly grueling because of the high overdose risk, the intensity of withdrawal, and the frequent co-occurrence of trauma and chronic pain.
The Rewards That Keep Them Going
Yet this field also delivers rewards that are hard to find elsewhere. Watching a client hit a recovery milestone, whether it is 30 days sober, reunifying with children, or simply showing up for a session after a relapse, provides a sense of purpose that counselors consistently describe as the primary reason they stay. The therapeutic alliance itself becomes a source of meaning: being the person who holds hope when a client cannot yet hold it for themselves. Counselors also point to the measurable community impact, seeing overdose rates decline in areas with robust treatment access and knowing their daily work contributes to that shift. With 17% projected job growth through 2034, the demand for professionals who can do this work is only increasing.4
Self-Care That Actually Moves the Needle
The strategies that practicing counselors recommend go beyond generic wellness advice. Clinical supervision is the backbone of emotional processing, not just a training requirement.3 It is the space where counselors unpack countertransference, receive validation, and regain perspective after difficult sessions. Peer support, whether through structured consultation groups or informal debriefing with coworkers, provides a buffer against isolation. Physical activity, even a brief walk between sessions, helps discharge the somatic tension that accumulates during intense clinical work. Finally, setting firm boundaries around after-hours availability protects recovery time and models healthy limits for clients. Structural changes matter too, including paid internships and clearer career ladders, but the daily practice of intentional self-care determines whether a counselor can sustain the work long enough to make the difference that drew them to the field.2 If you are still exploring whether this path is right for you, learning how to become a substance abuse counselor can help you weigh the demands against the deep professional rewards.
In addiction counseling, clinical supervision isn't just a box to check for licensure: it's the most consistently cited protective factor against burnout. It offers a dedicated, confidential space to process the vicarious trauma of hearing clients' darkest moments, recalibrate your clinical judgment, and build the emotional stamina needed to sustain this work long-term. For a field with high turnover, supervision is not a luxury; it's a lifeline.
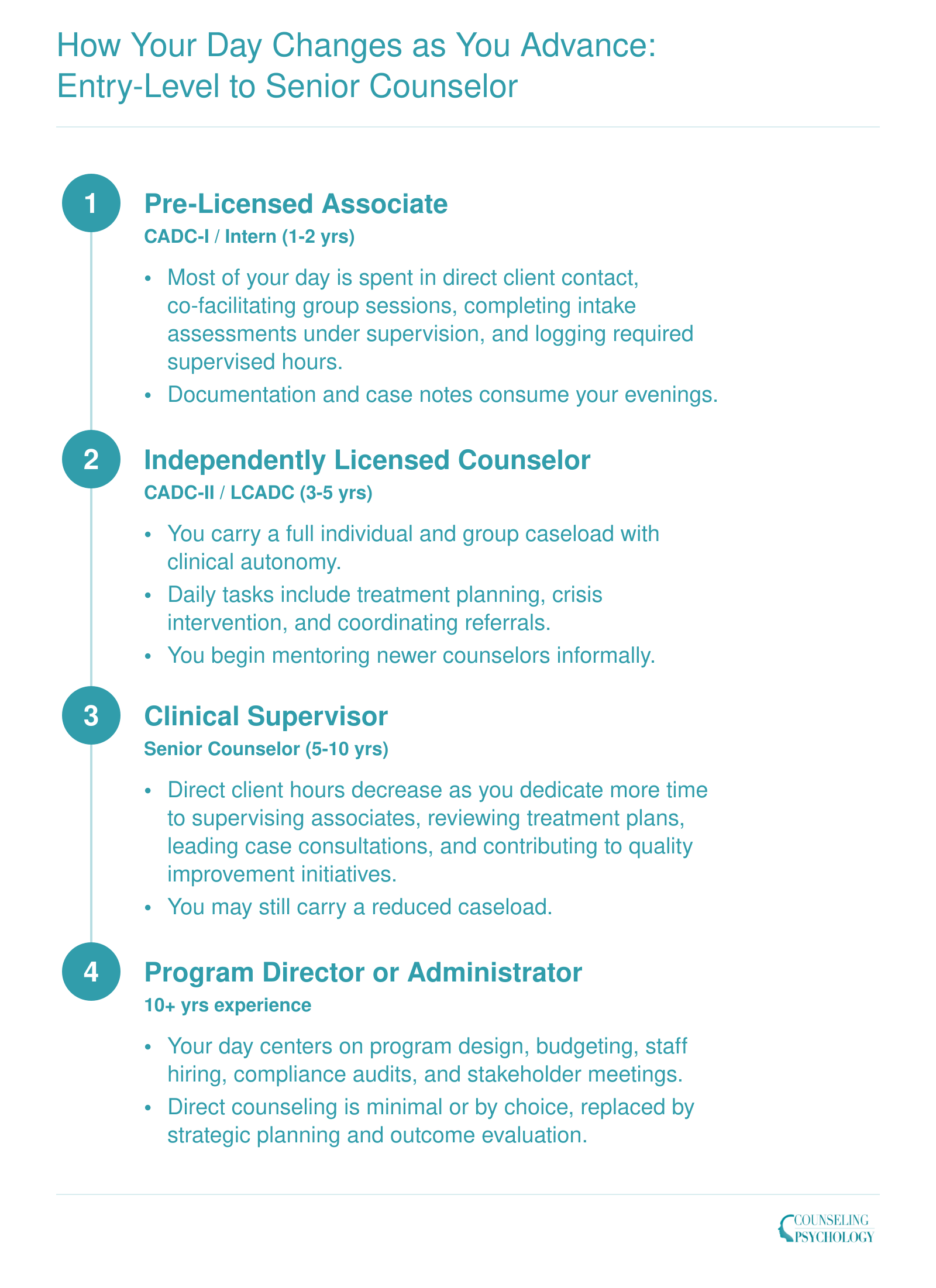
How Your Day Changes as You Advance: Entry-Level to Senior Counselor
Your daily routine as a substance abuse counselor shifts dramatically as you gain experience and credentials. Early career work is heavily clinical, but leadership responsibilities gradually replace direct client hours with supervision, program design, and administrative oversight.
Substance Abuse Counselor Salary and Job Outlook
Compensation for substance abuse, behavioral disorder, and mental health counselors varies by setting, experience, and geography. The table below pairs available national wage data with the occupation's projected growth rate so you can weigh both earning potential and long-term demand. The Bureau of Labor Statistics projects 17% job growth for this occupational group between 2024 and 2034, which is substantially faster than the average for all occupations. That projection reflects sustained demand driven by expanded insurance coverage for behavioral health services, ongoing substance use crises, and a broader cultural shift toward treating addiction as a medical condition rather than a moral failing. Keep in mind that counselors working in inpatient facilities, hospitals, or government agencies often earn more than those in outpatient community settings, and credentials such as state licensure or national certification (like the MAC or CASAC) can push salaries toward the higher end of the range. Program-level earnings data for specific degree pathways in this field are not yet widely available, so the figures below reflect the broader occupational category as reported by BLS.
| Metric | National Figure | Source |
|---|---|---|
| BLS Occupational Code | 21-1018 | Bureau of Labor Statistics |
| Projected Job Growth (2024 to 2034) | 17% | Bureau of Labor Statistics |
| Growth Comparison to All Occupations | Significantly faster than average | Bureau of Labor Statistics |
Frequently Asked Questions About Substance Abuse Counselor Workdays
These are some of the most common questions prospective counselors ask about the day-to-day realities of addiction counseling work. Each answer draws on the details covered throughout this article.