What you’ll learn in this article…
- BLS projects a 17% increase in community mental health counselor jobs from 2024 to 2034, adding roughly 42,000 positions.
- Most counselors need five to seven years from first college class to independent licensure in community settings.
- The national median wage for substance abuse, behavioral disorder, and mental health counselors sits near $53,710, though top metros pay considerably more.
- NHSC loan repayment can eliminate student debt for counselors who commit to serving underserved communities.
Roughly 160 million Americans live in federally designated Mental Health Professional Shortage Areas, yet the pipeline of licensed counselors entering community-based settings has not kept pace with that need. The gap is sharpest in rural counties, tribal lands, and low-income urban neighborhoods where public funding covers care that private insurance often does not.
Community mental health counselors work inside that gap. They provide assessment, crisis intervention, case management, and ongoing therapy to populations that include people experiencing poverty, serious mental illness, substance use disorders, housing instability, and trauma. Their employers are primarily publicly funded: community mental health centers, federally qualified health centers, corrections systems, schools, and nonprofit agencies. For a step-by-step look at entering this field, see our guide on how to become a community mental health counselor.
The BLS projects 17% job growth for this occupational category through 2034, more than double the average for all occupations. Still, high caseloads, modest starting salaries relative to the cost of a master's degree, and the demanding client mix mean the field selects for practitioners who enter with clear, realistic expectations rather than idealized ones. Those drawn to this work often find it among the most rewarding paths in counseling careers.
What Does a Community Mental Health Counselor Do?
CBT is the most widely adopted evidence-based practice class across community mental health agencies nationwide1, but the day-to-day reality of delivering it in a community setting looks nothing like the tidy therapy-room scenario most graduate programs depict. Community mental health counselors operate at the intersection of clinical work, social service coordination, and systemic advocacy, and their duties shift substantially depending on the setting.
Core Clinical Duties
A typical day begins with intake assessments for new clients who may present with co-occurring mental health and substance use disorders, housing instability, or involvement with the criminal justice system. From there, the work fans out:
- Individual therapy: Sessions draw on CBT, motivational interviewing, trauma-focused CBT for younger clients, and dialectical behavior therapy for those at higher risk. Community agencies often mandate specific evidence-based modalities tied to grant funding or Medicaid contracts, so counselors rarely have the luxury of an eclectic, choose-your-own approach.
- Group therapy: Psychoeducation groups, substance use recovery groups, and skills-based DBT groups are staples. Facilitating these efficiently is a core competency.
- Crisis intervention: Walk-in crises, suicidal ideation calls, and after-hours safety planning are routine rather than exceptional. If crisis work appeals to you, the role of a crisis intervention specialist shares many of the same competencies.
- Treatment planning and care coordination: Connecting clients to housing agencies, public benefits offices, primary care providers, and vocational rehabilitation programs is woven into nearly every case. IPS supported employment, for instance, is one of the most common psychosocial rehabilitation models for clients with serious mental illness.2
This is not a 50-minute-hour-and-done role. Sessions may be shorter, longer, or interrupted. Follow-up calls to case managers, probation officers, and family members fill the gaps between appointments.
How Duties Differ by Setting
The setting reshapes the counselor's entire workflow.
- Outpatient community mental health centers: Counselors carry structured caseloads of 30 to 60 or more clients. Documentation demands are heavy because Medicaid reimbursement requires detailed, diagnosis-linked progress notes for every encounter. Productivity benchmarks typically require 60 to 70 percent billable time, meaning roughly five to six hours of direct client contact in an eight-hour day, with documentation squeezed into the remaining time.
- Assertive community treatment (ACT) and mobile crisis teams: Work is field-based. Counselors visit clients in their homes, shelters, or hospital emergency departments. Hours are unpredictable, and caseloads are shared across a multidisciplinary team that may include a psychiatrist, nurse, and peer specialist.
- School-linked programs: Counselors consult with teachers and administrators, participate in IEP meetings, and deliver brief interventions to students. Sessions must fit within bell schedules, and documentation often needs to satisfy both the school district and the funding agency. Working with younger populations exposed to trauma may also overlap with childhood trauma counseling roles.
- Integrated primary care: Counselors embedded in medical clinics provide brief, targeted interventions (often 15 to 30 minutes) and execute warm handoffs from physicians who identify behavioral health concerns during routine visits. CBT and motivational interviewing are the dominant modalities here, applied in compressed formats.
The Documentation Reality
Most new counselors are caught off guard by the sheer volume of paperwork. Agencies funded through Medicaid, SAMHSA block grants, or state contracts require thorough clinical documentation for every billable service.3 When productivity expectations hover around 60 to 70 percent direct service time, the math leaves little breathing room. Writing a detailed progress note for each session, updating treatment plans on schedule, and completing required outcome measures can easily consume two or more hours each day. Graduate programs that teach note-writing as an afterthought leave their students at a disadvantage.
Evidence-Based Practices You Should Expect to Use
Community mental health agencies do not simply encourage evidence-based treatment; funders often require it. The most commonly implemented models nationally include:1
- CBT and its adaptations for depression, anxiety, and substance use
- Trauma-focused CBT, the leading evidence-based approach for children exposed to trauma
- Motivational interviewing, a cross-cutting technique applied to substance use, treatment engagement, and health behavior change
- DBT, particularly for clients with higher-risk presentations
- IPS supported employment for clients with serious mental illness pursuing vocational goals
- Family-based evidence-based practices and illness management and recovery (IMR) models
SAMHSA has consistently emphasized CBT, trauma-focused interventions, motivational interviewing, supported employment, and assertive community treatment in its strategic priorities through 2026.2 If you enter this field, fluency in at least two or three of these approaches is not optional; it is a baseline expectation from day one.
Community Mental Health vs. Private Practice Counseling
Choosing between community mental health and private practice counseling means weighing mission and stability against autonomy and income potential. Both paths lead to licensure as a mental health professional, but they differ sharply in daily operations, compensation, client populations, and career trajectory. Understanding these differences early helps you align your training and expectations with the realities of each practice setting.
Pay and Benefits
Salary data from the Bureau of Labor Statistics (BLS) shows that mental health counselors, whether in community or private settings, earned a national median wage of $53,710 in 2023. Private practitioners, often classified under clinical and counseling psychologists when holding advanced degrees, reported higher median earnings at $96,100 nationally in 2023. However, private-practice counselors operating without doctoral credentials typically earn closer to the general counselor median during their first years and face higher overhead costs for office space, billing software, malpractice insurance, and marketing that salaried community roles do not require. The American Counseling Association (ACA) has periodically surveyed its members and found that private practitioners in established practices report higher gross income but also describe longer workweeks and greater financial variability year-to-year compared to salaried community counselors who receive health insurance, retirement matching, paid time off, and loan-forgiveness eligibility under programs like Public Service Loan Forgiveness (PSLF).
Client Base and Autonomy
Community mental health centers serve diverse, often underserved populations: clients with serious mental illness, substance-use disorders, unstable housing, and Medicaid or no insurance. Caseloads are higher, sessions may be shorter (30 to 45 minutes), and documentation requirements are intensive to meet state and federal funding mandates. Counselors who want to deepen their competence with these populations may also benefit from multicultural counseling training. Private practice counselors enjoy greater control over scheduling, session length, modality (in-person, telehealth, group), and client selection. Many private practitioners focus on specific niches such as anxiety, trauma, or couples work, and some do not accept insurance panels, allowing them to set their own fees and reduce administrative burden.
Career Stage and Licensing Pathways
Most states require supervised post-degree hours for full licensure as a Licensed Professional Counselor (LPC) or Licensed Mental Health Counselor (LMHC). Community mental health agencies are the largest employers of provisionally licensed counselors, offering structured supervision, diverse clinical exposure, and pathways to independent licensure. Private practice typically requires full licensure from the outset, so many counselors spend two to three years in community or agency settings before transitioning to solo or group practice. The National Board for Certified Counselors (NBCC) notes that counselors who hold the National Certified Counselor (NCC) credential report slightly higher salaries and faster progression to supervisory roles, regardless of practice setting.
Long-Term Trajectories
Peer-reviewed comparisons between community mental health and private practice show that private practitioners report higher job satisfaction related to autonomy and flexibility, while community counselors cite mission alignment and team support as primary satisfactions. Burnout rates are elevated in both settings, but for different reasons: community counselors face heavier caseloads and administrative demands, while solo practitioners report isolation and financial stress. The availability of BIPOC therapists remains a concern in both settings, as workforce diversity affects access and outcomes for underserved communities. Many experienced counselors blend both models, maintaining part-time community roles for stable income and benefit coverage while building a limited private caseload on evenings or weekends.
Questions to Ask Yourself
Education and Licensure Requirements
A clinical mental health counseling master's and a master's in social work (MSW) represent two distinct routes into community mental health work. Each has its own professional culture, credential endpoint, and licensure track, yet both open doors to nearly the same job postings at community health centers, crisis agencies, and nonprofits. Understanding which path fits your goals starts with knowing what the credential journey actually looks like.
The Standard Academic Pathway
Most counselors begin with any bachelor's degree, then enter a graduate program in clinical mental health counseling. The target is a 60-credit-hour master's from a program accredited by CACREP (the Council for Accreditation of Counseling and Related Educational Programs). That credit threshold is not arbitrary: many state licensing boards require it explicitly, and programs that fall short can leave graduates ineligible to sit for licensure in certain states. You can compare options through online clinical mental health counseling programs to find CACREP-accredited degrees that meet your state's requirements.
MSW programs follow a parallel track. Social work degrees are governed by CSWE accreditation rather than CACREP, but a number of states formally accept MSW holders as eligible for community mental health counselor licensure, broadening the talent pipeline considerably.
Supervised Hours and the Licensure Exam
After graduation, every candidate completes supervised post-graduate clinical hours before applying for full licensure. The range is wide: state requirements typically fall between 2,000 and 4,000 hours, with the exact number, supervision ratio, and qualifying supervisor credentials spelled out in each state's statutes. Completing those hours at a community mental health agency is common, which means many counselors are already doing the job before they hold the final credential.
The two main licensure exams are the NCE (National Counselor Examination) and the NCMHCE (National Clinical Mental Health Counseling Examination). Which exam a state requires, or whether it accepts both, varies by jurisdiction. Reviewing counseling licensure requirements by state early in your planning can save months of frustration later.
Decoding the Credential Alphabet
Once licensed, counselors run into a confusing patchwork of titles:
- LPC: Licensed Professional Counselor (used in many Southern and Midwestern states)
- LMHC: Licensed Mental Health Counselor (common in New York, Florida, and the Northwest)
- LCPC: Licensed Clinical Professional Counselor (Illinois, Idaho, and others)
- LPCC: Licensed Professional Clinical Counselor (California, Ohio, and several more)
These titles are functionally equivalent. They describe the same scope of practice achieved through the same master's-level training and supervised hours. For a full breakdown, the guide to counseling licensure acronyms explains every credential in detail. The difference is purely jurisdictional, which creates real headaches for counselors who relocate. Someone licensed as an LMHC in Massachusetts who moves to Texas must navigate that state's LPC requirements, sometimes including additional coursework or re-examination. Checking the licensure requirements page for your target state before you enroll in a program is a smart early step.
Why CACREP Accreditation Matters
CACREP accreditation is the most reliable signal of licensure portability. When a program meets CACREP standards, its curriculum has been benchmarked against a national framework, and most state boards recognize it without requiring supplemental coursework. Some states are moving toward requiring CACREP accreditation outright, so choosing a non-CACREP program to save time or tuition can create complications down the road.
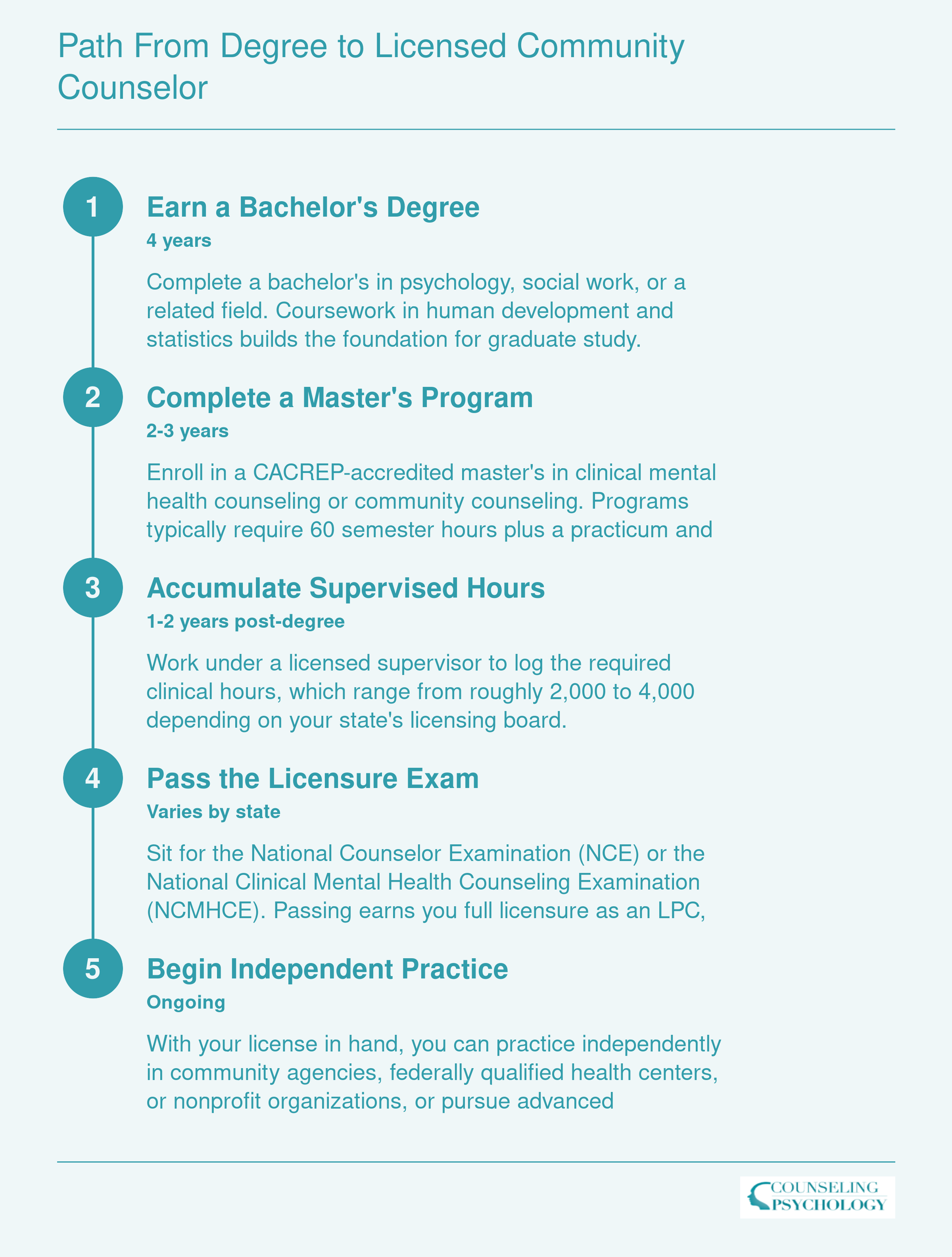
Path from Degree to Licensed Community Counselor
Most community mental health counselors spend roughly five to seven years moving from their first college class to independent practice. Here is how that timeline typically breaks down.
Community Mental Health Counselor Salary by State
Salaries for community mental health counselors vary significantly by geography. The table below draws from BLS data for substance abuse, behavioral disorder, and mental health counselors (SOC 21-1018), the occupational category that captures most community counseling roles. Keep in mind that cost of living, state funding for behavioral health, and licensure requirements all influence these figures.
| State | Total Employment | 25th Percentile | Median Salary | 75th Percentile | Mean Salary |
|---|---|---|---|---|---|
| Alaska | 1,060 | $63,690 | $79,220 | $96,940 | $88,870 |
| New Mexico | 2,070 | $55,060 | $70,770 | $80,840 | $71,010 |
| Oregon | 6,410 | $56,290 | $69,660 | $84,970 | $72,860 |
| North Dakota | 1,180 | $50,810 | $66,450 | $75,120 | $68,220 |
| District of Columbia | 980 | $47,980 | $66,140 | $83,040 | $71,200 |
| Utah | 4,720 | $42,210 | $65,920 | $94,630 | $71,890 |
| Idaho | 2,130 | $48,570 | $65,240 | $78,100 | $65,290 |
| New Jersey | 14,640 | $51,170 | $64,710 | $84,690 | $75,900 |
| Nebraska | 1,980 | $46,900 | $64,410 | $81,210 | $66,690 |
| Washington | 13,150 | $52,070 | $64,220 | $80,440 | $70,230 |
| Arizona | 8,970 | $50,650 | $63,830 | $79,990 | $67,890 |
| Connecticut | 6,470 | $49,120 | $62,960 | $77,610 | $66,920 |
| Wisconsin | 9,450 | $50,870 | $62,470 | $77,800 | $70,180 |
| New York | 22,450 | $50,880 | $62,070 | $76,680 | $69,290 |
| Wyoming | 840 | $42,610 | $61,640 | $79,830 | $65,650 |
| California | 63,110 | $47,650 | $61,310 | $90,370 | $72,530 |
| Maine | 1,610 | $48,360 | $60,970 | $73,510 | $64,050 |
| Iowa | 3,030 | $49,170 | $60,880 | $78,830 | $65,960 |
| Texas | 19,520 | $47,600 | $60,630 | $76,390 | $67,920 |
| Vermont | 1,150 | $52,890 | $60,410 | $67,670 | $63,060 |
| Illinois | 18,170 | $47,640 | $59,570 | $81,250 | $69,010 |
| Michigan | 11,090 | $42,480 | $59,530 | $74,360 | $61,960 |
| Nevada | 2,240 | $46,960 | $59,470 | $76,260 | $64,430 |
| Colorado | 13,670 | $47,750 | $59,190 | $78,350 | $66,280 |
| Massachusetts | 17,950 | $47,120 | $59,030 | $73,000 | $64,020 |
| Minnesota | 7,910 | $49,880 | $58,720 | $64,370 | $59,020 |
| Montana | 1,900 | $39,220 | $58,660 | $68,360 | $57,350 |
| Oklahoma | 4,460 | $44,320 | $58,610 | $78,710 | $62,220 |
| New Hampshire | 3,100 | $48,310 | $58,520 | $73,770 | $61,100 |
| Virginia | 16,860 | $47,530 | $58,410 | $76,530 | $63,630 |
| Pennsylvania | 26,510 | $46,910 | $58,320 | $72,800 | $61,040 |
| Maryland | 8,180 | $48,980 | $57,820 | $70,990 | $68,830 |
| Kansas | 2,410 | $45,050 | $57,760 | $67,540 | $59,530 |
| Ohio | 16,690 | $47,370 | $56,990 | $67,470 | $59,960 |
| Florida | 24,680 | $46,640 | $56,830 | $67,700 | $60,480 |
| Missouri | 7,500 | $42,930 | $56,640 | $66,810 | $58,230 |
| North Carolina | 8,930 | $47,460 | $56,470 | $68,470 | $60,440 |
| Georgia | 8,680 | $46,150 | $55,320 | $71,980 | $61,250 |
| Hawaii | 1,580 | $49,630 | $54,390 | $76,220 | $75,610 |
| South Dakota | 1,510 | $46,260 | $53,400 | $59,770 | $55,890 |
| Kentucky | 8,030 | $39,560 | $51,790 | $75,310 | $58,190 |
| South Carolina | 4,680 | $40,480 | $50,720 | $65,770 | $55,450 |
| Arkansas | 2,860 | $37,280 | $49,990 | $69,630 | $58,960 |
| Rhode Island | 1,560 | $42,550 | $49,770 | $67,370 | $58,860 |
| Delaware | 1,240 | $41,630 | $49,680 | $65,270 | $56,120 |
| Indiana | 10,400 | $41,860 | $49,280 | $62,780 | $54,630 |
| Alabama | 3,340 | $40,480 | $48,880 | $58,540 | $52,120 |
| Tennessee | 7,310 | $36,910 | $48,170 | $60,900 | $51,480 |
| Mississippi | 2,220 | $37,830 | $46,810 | $56,800 | $54,120 |
Highest-Paying Metro Areas for Community Counselors
Geography plays a major role in community mental health counselor salary. The table below ranks the top 10 highest-paying metropolitan areas by median annual wage for substance abuse, behavioral disorder, and mental health counselors, according to BLS data. Keep in mind that metros with the largest paychecks often carry a higher cost of living, so weigh local expenses against the raw numbers before relocating for a position.
| Metropolitan Area | Total Employment | Median Annual Wage | 25th Percentile | 75th Percentile | Mean Annual Wage |
|---|---|---|---|---|---|
| San Francisco, Oakland, Fremont (CA) | 8,080 | $72,950 | $54,110 | $108,410 | $83,140 |
| Portland, Vancouver, Hillsboro (OR, WA) | 3,640 | $71,530 | $60,230 | $86,150 | $75,920 |
| Sacramento, Roseville, Folsom (CA) | 3,570 | $69,510 | $48,860 | $99,790 | $78,880 |
| Seattle, Tacoma, Bellevue (WA) | 7,040 | $65,290 | $53,890 | $81,230 | $71,930 |
| New York, Newark, Jersey City (NY, NJ) | 23,790 | $64,900 | $52,770 | $81,680 | $75,500 |
| Houston, Pasadena, The Woodlands (TX) | 4,230 | $64,140 | $49,340 | $76,890 | $68,820 |
| Phoenix, Mesa, Chandler (AZ) | 6,830 | $63,990 | $50,190 | $82,350 | $67,740 |
| Washington, Arlington, Alexandria (DC, VA, MD, WV) | 7,590 | $63,170 | $50,280 | $83,780 | $73,210 |
| Chicago, Naperville, Elgin (IL, IN) | 14,010 | $61,150 | $47,980 | $83,770 | $70,920 |
| Riverside, San Bernardino, Ontario (CA) | 5,170 | $60,860 | $47,490 | $78,210 | $66,800 |
National Salary Snapshot for Mental Health Counselors
Across roughly 440,380 employed substance abuse, behavioral disorder, and mental health counselors nationwide, pay varies considerably by experience, setting, and location. The figures below reflect the national wage distribution reported by the Bureau of Labor Statistics.

Job Outlook and Demand for Community Counselors
The Bureau of Labor Statistics projects a 17% increase in jobs for substance abuse, behavioral disorder, and mental health counselors between 2024 and 2034, a rate much faster than the average for all occupations.1 This surge translates into roughly 42,000 new positions opening up each year, on average, over the decade.
Strong Job Growth Driven by Systemic Demand
Several structural forces are fueling the need for community-based counselors. Expanded Medicaid behavioral health mandates now require coverage for mental health and substance use services at parity with medical care, opening up access for millions. The post-pandemic demand surge has not subsided; communities are still grappling with elevated rates of anxiety, depression, and substance use, while public awareness and destigmatization continue to drive more people to seek help. At the same time, an aging workforce means many experienced counselors are approaching retirement, creating substantial replacement openings alongside new role growth. For a deeper look at these dynamics, our analysis of the mental health workforce shortage breaks down the numbers by region and specialty.
Widespread Shortages Create Immediate Opportunities
Federal data highlight the scale of unmet need. The Health Resources and Services Administration designates Mental Health Professional Shortage Areas (HPSAs) across the country. Currently, over 160 million Americans live in areas with inadequate access to mental health providers. Community mental health centers, nonprofit clinics, and public agencies in these regions are actively recruiting counselors to fill critical gaps. New graduates who are willing to work in HPSAs often find a favorable job market with quicker hiring timelines and, in some cases, signing bonuses or relocation assistance.
Financial Incentives for Working in Underserved Areas
To attract counselors to high-need communities, several loan repayment and grant programs are available. The National Health Service Corps Loan Repayment Program offers up to $75,000 in loan forgiveness for a three-year commitment in an approved shortage area. Many states run their own loan repayment programs that mirror or supplement this federal support. Additionally, HRSA Behavioral Health Workforce Education and Training grants fund positions in community-based settings, sometimes covering tuition or providing stipends during a counselor's training. Understanding realistic counselor salary expectations alongside these incentives can help you evaluate whether this career path is financially sustainable. These programs make it feasible to pursue work that, while demanding, offers long-term stability and the chance to make a tangible difference.
Licensed behavioral health providers are eligible for the National Health Service Corps Loan Repayment Program, which can significantly reduce or eliminate student debt for clinicians who commit to working in underserved communities. For the latest participation figures and total award amounts, the NHSC annual report on HRSA.gov is the most reliable source.
Work Settings and Client Populations
The typical workday of a community mental health counselor looks nothing like the private practice model: it unfolds in publicly funded clinics, school hallways, mobile vans, and correctional facilities where the need for accessible mental health care is most acute.
Five Pillars of Community Mental Health Service
Community counselors serve in settings that prioritize access over profit, often working within a patchwork of federal, state, and local funding streams. Major employers include:
- Community mental health centers: The backbone of the system, these centers offer sliding-scale fees and accept Medicaid, providing therapy, case management, and crisis services regardless of a client's ability to pay.
- Federally Qualified Health Centers (FQHCs): Integrated behavioral health models embed counselors alongside primary care providers, allowing for warm hand-offs and coordinated treatment of physical and mental health.
- Mobile crisis teams: Counselors ride alongside paramedics or police alternative responders to de-escalate psychiatric emergencies in homes, shelters, and public spaces, diverting individuals from emergency rooms and jails.
- School-based mental health programs: Placed directly in K-12 schools, these counselors offer on-site therapy, teacher consultation, and family outreach, removing transportation and scheduling barriers for children and teens.
- Correctional and re-entry programs: Counselors work inside jails and prisons or with justice-involved individuals returning to the community, addressing trauma, substance use, and criminogenic thinking.
Urban Intensity vs. Rural Breadth
The practice of community counseling differs dramatically by geography. Urban settings concentrate populations with complex needs, leading to high caseloads and constant demand. However, urban counselors benefit from large interdisciplinary teams, specialized programs for specific populations (such as homeless youth or refugees), and robust referral networks for housing, medical care, and substance abuse treatment. In contrast, rural community counselors often function as the sole mental health provider for an entire county. They manage a broader scope of practice out of necessity, covering crisis response, substance use, geriatric counseling, and child and adolescent therapy, but face professional isolation, long travel distances to see clients, and a scarcity of psychiatrists or residential facilities for higher levels of care.
A Clinically Complex Clientele
The client mix in community mental health departs significantly from the predominantly anxiety and depression caseloads common in private practice. Counselors regularly work with serious mental illnesses such as schizophrenia and bipolar I disorder, often compounded by co-occurring substance use disorders. Trauma-exposed children and families, including those involved in the child welfare system, make up a large share of school-based and agency caseloads. Professionals drawn to this population may also explore childhood trauma counseling as a focused career path. Court-mandated clients add another layer, requiring counselors to balance therapeutic alliance with legal reporting duties. This clinical diversity demands proficiency in a wide range of evidence-based approaches, from motivational interviewing and trauma-focused cognitive behavioral therapy to illness management and recovery models.
Telehealth Transforms Access
The rapid expansion of telehealth has fundamentally altered community mental health workflows. For rural counselors, video sessions have become a lifeline, reducing no-show rates tied to transportation problems and allowing more frequent contact with isolated clients. In urban settings, telehealth enables hybrid schedules that can lessen burnout and extend service hours to evenings and weekends. However, the digital divide remains a barrier: clients experiencing homelessness or severe poverty may lack reliable internet or private spaces for sessions, forcing programs to maintain in-person options while navigating new parity and licensing regulations across state lines. Counselors now find themselves navigating both virtual and in-person care pathways, often within the same day.
Challenges, Burnout, and Rewards of Community Mental Health Work
Sustained enthusiasm versus cautious realism: both are present among community mental health counselors, and both are warranted. This field offers some of the most meaningful clinical work available, and it also asks more of its practitioners than most counseling settings do. Going in with a clear picture of both sides is not pessimism; it is preparation.
The Real Weight of the Work
Caseload sizes in community mental health settings typically run between 25 and 40 active clients, and productivity expectations usually require 22 to 30 billable hours per week.1 Many agencies target 60 to 70 percent of a counselor's weekly hours as billable time, which leaves the remainder crowded with documentation, treatment planning, coordination, and administrative tasks that expand to fill every available gap.2
Those structural pressures compound over time. Burnout prevalence among community mental health counselors sits at roughly 51 percent, according to recent workforce data, and national figures for therapists broadly show that about 54 percent report burnout and 67 percent experience burnout symptoms at least occasionally.3 Annual staff turnover at community mental health agencies ranges from 30 to 60 percent, a rate that reflects not individual weakness but systemic underfunding, compensation that lags behind the level of training required, and the accumulated weight of treating high-acuity populations without adequate organizational support.2
Vicarious trauma deserves its own acknowledgment here. Working daily with clients in crisis, poverty, and trauma takes a toll that does not resolve by clocking out. Framing these outcomes as personal failure misses the point. They are predictable responses to structural conditions, and they are why agency culture matters as much as job title.
Why Counselors Stay
Despite the pressures, retention exists in this field for real reasons. Community counselors work with clients who, without public mental health services, would have no access to care at all. That reality creates a sense of purpose that many clinicians describe as irreplaceable. The clinical exposure is also genuinely accelerated: complex presentations, co-occurring disorders, and crisis intervention specialist work build competency faster than lower-acuity settings typically allow. Team culture in well-run agencies provides peer support and shared mission that private practice solo work rarely replicates.
For those considering this path, our guide on how to become a community mental health counselor outlines the education, licensure, and training steps involved.
What to Look for Before You Accept a Position
Protective factors are real, but they are not uniformly distributed across agencies. Before accepting an offer, ask direct questions:
- Caseload size: What is the average active caseload for a full-time clinician?
- Supervision quality: How often does individual clinical supervision occur, and is it protected time or routinely cancelled?
- Administrative support: Is documentation time built into the schedule, or is it expected off the clock?
- Turnover history: How long have current staff members been in their roles?
- Organizational culture: How does leadership respond when clinicians flag unsustainable workloads?
Agencies vary considerably on every one of these dimensions. A setting with manageable caseloads, genuine clinical supervision, and a culture that treats burnout as an organizational problem rather than a personal one produces meaningfully different outcomes for both counselors and clients. Researching an employer with the same rigor you bring to clinical work is not excessive caution; it is part of a sustainable career strategy.
Before accepting a community mental health position, ask about turnover rates, clinical supervision budgets, and productivity targets. High turnover, no supervision funding, or unrealistic caseloads are red flags for burnout. Smart job seekers raise these questions early, using the responses to identify agencies that invest in sustainable workloads and professional growth. Avoid employers who cannot or will not discuss these openly.
How to Launch Your Community Mental Health Career
Launching a career in community mental health requires more than a degree. It demands strategic choices in training, employment, and professional development.
Building Your Experience While in School
The most direct route into community mental health begins with your practicum and internship placements. Selecting sites such as community clinics, crisis centers, or nonprofit counseling agencies gives you hands-on experience with the populations and challenges you will encounter daily. These placements also introduce you to potential employers; many agencies hire from their intern pool. Treat every placement as an extended interview, demonstrating reliability and cultural competence often leads directly to a job offer. Prioritize sites that offer direct client contact under robust supervision, exactly the skill set community employers value most.
Evaluating Potential Employers
After graduation, the job search becomes a two-way assessment. Before accepting a position, gather information that reveals an agency's work environment and sustainability. Use the following checklist in interviews or site visits:
- Caseload size: What is the average number of active clients per counselor? High caseloads can indicate productivity pressure.
- Supervision ratio: How many counselors are assigned to each clinical supervisor? Adequate support reduces burnout risk.
- Staff turnover rate: Ask about retention. Frequent departures signal systemic stress.
- Productivity expectations: Are there quotas for billable hours or client contacts? Understand what a typical week requires.
- Loan repayment eligibility: Determine whether the agency is an NHSC-approved site. Loan repayment programs can offset lower salaries in community settings.
Mapping Your Career Progression
Community mental health experience opens multiple advancement pathways, not just linear clinical promotions. Typical roles progress from direct service counselor to clinical supervisor, then to program director overseeing service delivery. Seasoned professionals often move into agency leadership or executive director positions, or pivot to policy and advocacy roles within state behavioral health authorities. Public health departments and grant-funded research initiatives also value the on-the-ground perspective that community work provides. The credibility gained from direct community work often proves invaluable when transitioning into administration or system-level change.
Expand Your Network and Skillset
Professional community and specialized credentials enhance both your practice and career mobility. Join the American Counseling Association's Community Counseling interest network and your state mental health counselors association; many offer mentorship programs, job boards, and continuing education tailored to community settings. To stand out, pursue certifications in high-demand areas: trauma-focused therapy, substance use disorder treatment, or child and adolescent counseling. A polished counselor resume that highlights these specialties will strengthen your candidacy. These credentials not only improve client outcomes but also match the most pressing needs in community settings, making you a more competitive candidate for advancement.
Frequently Asked Questions About Community Mental Health Counseling
Below are answers to some of the most common questions prospective community mental health counselors ask. Where possible, each answer references data and context covered in earlier sections of this guide.