Key Takeaways
- Becoming a physiatrist requires 12 to 14 years of education and training after high school.
- Both MD and DO graduates match into PM&R residencies at high rates, often exceeding 95% fill.
- Pain medicine and interventional spine physiatrists consistently earn the highest salaries within the specialty.
- Medical school debt typically ranges from $200,000 to $300,000, though median physician earnings exceed $250,000.
Physiatrists are fully licensed physicians who restore function without surgery, distinguishing their role from orthopedists and surgeons. The most common question about entering the field has a straightforward answer: physiatrists go to medical school, and the full training pipeline spans 12 to 14 years after high school.
This guide lays out the path step by step, from the bachelor's degree to board certification, with salary benchmarks and match competitiveness statistics highlighted at each major checkpoint. PM&R residency fill rates consistently exceed 95%, reflecting strong demand, while median compensation crosses $250,000 nationally. That figure shifts sharply by subspecialty and practice setting, so the sections ahead break down exactly what to expect at every stage.
What Is a Physiatrist?
With an aging population and a growing emphasis on non-opioid pain management, physiatry is rapidly evolving into a cornerstone of multidisciplinary patient care.
The Non-Surgical Approach to Recovery
Physical Medicine and Rehabilitation (PM&R), commonly called physiatry, is a medical specialty that aims to restore function and improve quality of life for people with physical impairments or disabilities. Unlike surgical fields, physiatrists focus on non-operative treatments, using a combination of physical modalities, medications, and coordinated therapy plans to help patients regain independence after injury, illness, or chronic conditions. The core philosophy is treating the whole patient, not just the specific injury.
Conditions Physiatrists Treat
Physiatrists manage a wide range of neuromuscular and musculoskeletal conditions. Common patient populations include:
- Spinal cord injuries: Helping individuals adapt and maximize mobility.
- Traumatic brain injuries (TBI): Guiding cognitive and physical rehabilitation.
- Stroke recovery: Addressing motor deficits, speech challenges, and daily living skills.
- Musculoskeletal pain: Diagnosing and treating back, neck, and joint pain without surgery.
- Sports injuries: Designing return-to-play protocols and performance optimization.
- Amputee care: Overseeing prosthetic training and pain management.
A Day in the Life
A physiatrist's daily work is highly collaborative. They conduct thorough patient evaluations, often using electromyography (EMG) and nerve conduction studies to pinpoint nerve and muscle damage. They lead multidisciplinary rehabilitation teams that typically include physical therapists, occupational therapists, and speech-language pathologists. In addition to team coordination, physiatrists perform interventional procedures such as ultrasound-guided joint injections, nerve blocks, and trigger point injections. A large portion of their time is also spent developing long-term pain management plans that may include medication, therapeutic exercise, and assistive device prescriptions. Professionals interested in the broader rehabilitation landscape, including roles like vocational rehabilitation counselors, often collaborate closely with physiatrists to support patients' return to work and daily functioning.
Physiatrist vs. Physical Therapist
It's easy to confuse physiatrists with physical therapists, but the roles are distinct. Physiatrists are fully licensed physicians who hold an MD or DO degree and have completed a four-year residency in PM&R. This medical training allows them to diagnose complex conditions, prescribe medications, and perform procedures. Physical therapists (DPTs) are highly skilled doctoral-level professionals who implement rehabilitation exercises and manual therapy but cannot diagnose medical conditions or prescribe medication. The physiatrist often directs the overall treatment plan that a physical therapist carries out.
How Long Does It Take to Become a Physiatrist?
The path from freshman year to practicing physiatrist spans roughly 12 to 14 years. That makes PM&R's training pipeline about one year longer than internal medicine but still shorter than most surgical specialties. Exceptional students enrolled in combined BS/MD or BS/DO early-acceptance programs can trim one to two years off the undergraduate phase, reaching residency sooner.
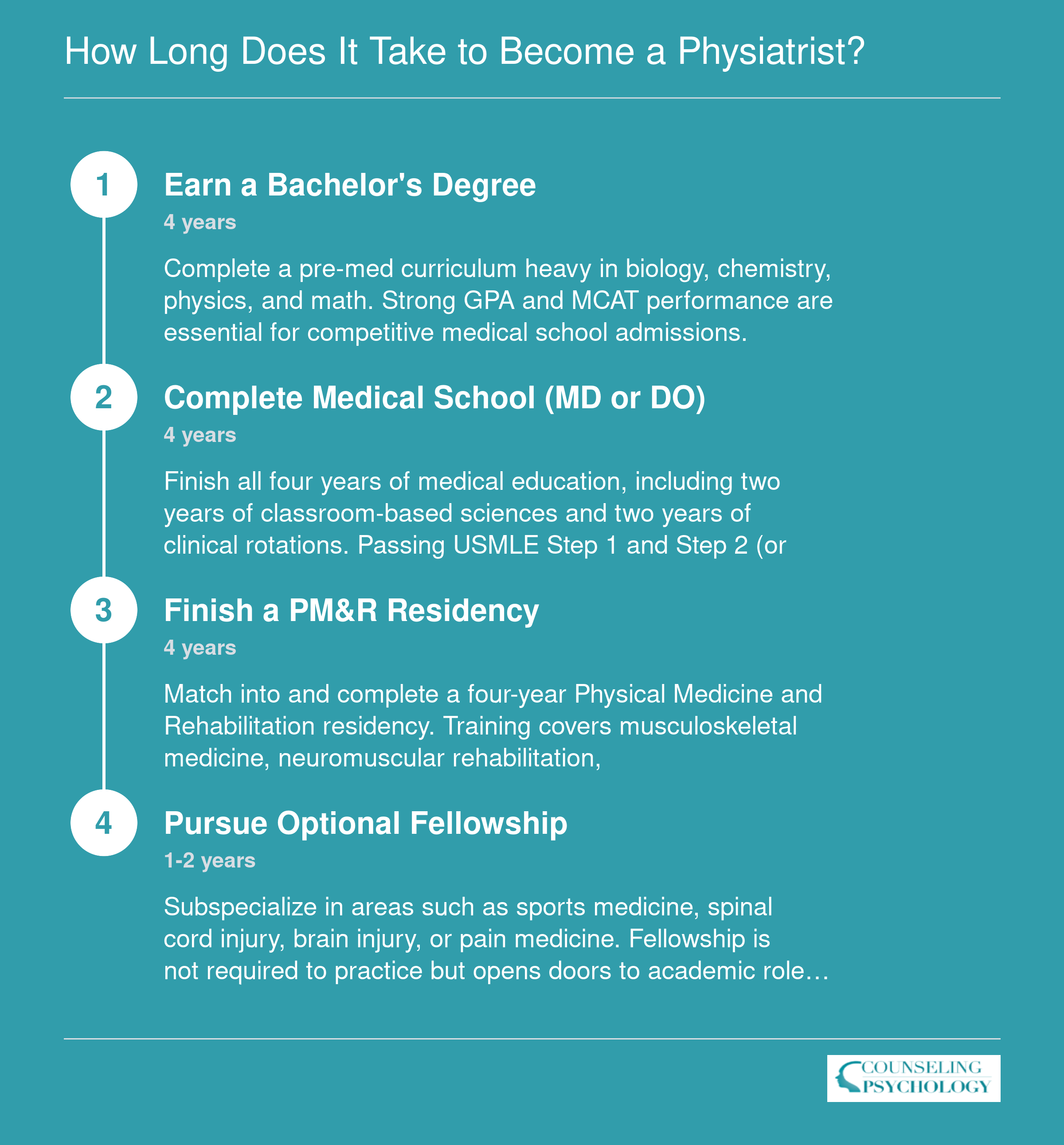
Step 1: Earn a Bachelor's Degree
While some future physiatrists choose a biology or kinesiology major, others pursue degrees in psychology or even the humanities. Medical schools accept any undergraduate field as long as essential prerequisites are completed. A strong academic foundation and purposeful clinical experiences matter far more than the name of your major. This step sets the stage for medical school admission and a career in physical medicine and rehabilitation (PM&R).
Choosing a Major or Degree Path
Physiatry does not require a specific pre-med major. Admissions committees at allopathic (MD) and osteopathic (DO) programs value diverse academic backgrounds. Common choices, such as biology, neuroscience, kinesiology, exercise science, and health sciences, naturally align with medical school prerequisites and are widely available at most four-year institutions. However, an increasing number of successful applicants major in psychology, sociology, engineering, or the humanities. What unites them is deliberate planning: early identification of required coursework, sustained academic performance, and extracurricular engagement that demonstrates genuine interest in rehabilitation medicine.
If your bachelor's program is outside the sciences, work closely with a pre-health advisor to ensure your schedule accommodates all prerequisites without delaying graduation. Some students pair a non-science major with a minor in chemistry or biology to streamline the process. The flexibility of this step lets you play to your strengths; just be strategic about fitting in the core science courses.
Prerequisite Courses and GPA Targets
Medical schools expect a coherent set of foundational sciences, typically including: - Biology: Two semesters with lab, covering cell biology, genetics, and physiology. - General Chemistry: Two semesters with lab. - Organic Chemistry: Two semesters with lab; some schools now accept a semester of organic chemistry plus a semester of biochemistry. - Physics: Two semesters with lab. - Biochemistry: One semester (often strongly recommended if not explicitly required). - English: Two semesters of writing-intensive coursework. - Statistics: One semester of biostatistics or general statistics, increasingly valued for evidence-based practice.
A cumulative GPA of 3.5 or higher is competitive at most MD-granting schools; DO programs may have slightly lower averages but still reward academic rigor. Challenging upper-division science courses can both boost your science GPA and signal readiness for medical school intensity. If your GPA dips early, an upward trend and strong post-baccalaureate work can mitigate concerns.
Gaining Early Clinical Exposure Specific to PM&R
Shadowing and hands-on experience within rehabilitation settings confirm your interest and enrich your application narrative. Students interested in the broader rehabilitation field may also explore how to become a rehabilitation counselor to understand the allied professions physiatrists collaborate with. Seek opportunities to: - Shadow a physiatrist in an outpatient musculoskeletal clinic, inpatient rehab unit, or subacute care facility. Observing interdisciplinary team rounds, where physiatrists collaborate with physical therapists, occupational therapists, and speech-language pathologists, offers a nuanced view of the specialty. - Volunteer in inpatient rehabilitation units, often available through academic medical centers, VA hospitals, or community hospitals. These roles expose you to spinal cord injury, traumatic brain injury, stroke, and amputation populations, all core populations in PM&R. - Work part-time as a rehab aide or therapy technician. These positions, sometimes obtainable with a high school diploma and on-the-job training, build rapport with clinicians, provide direct patient contact, and strengthen medical school applications by demonstrating sustained commitment.
Document all experiences carefully; admissions committees look for longitudinal, meaningful involvement rather than one-off observations.
Planning MCAT Preparation
The Medical College Admission Test (MCAT) typically looms late in your junior year or early senior year, with most applicants sitting for it in the spring or summer before applying. Build a dedicated study period of 3 to 6 months alongside or after completing the core prerequisites. Average MCAT scores for accepted students cluster around 511 to 512, with competitive scores for top programs often exceeding 515. Start by reviewing the test's four sections (Biological and Biochemical Foundations, Chemical and Physical Foundations, Psychological/Social/Behavioral Foundations, and Critical Analysis and Reasoning Skills) and take a diagnostic exam early. Many students combine self-study resources such as review books and question banks with a prep course or study group. Reserve time for full-length practice exams; stamina and pacing are as critical as content knowledge. Integrating MCAT study into your daily routine while protecting extracurricular time prevents burnout and maintains perspective.
Questions to Ask Yourself
Step 2: Complete Medical School (MD or DO)
The choice between an allopathic (MD) and osteopathic (DO) medical degree involves balancing training philosophy with match outcomes, but in physical medicine and rehabilitation, both paths are equally viable and well-represented. DO graduates comprise a significant share of PM&R residents, so students should select the program that best fits their learning style and career goals.
MD vs. DO: Both Pathways Lead to PM&R
Allopathic medical schools confer the MD degree and emphasize a disease-focused curriculum, while osteopathic programs award the DO degree and add training in osteopathic manipulative medicine. Both degrees prepare you for residency and board certification. NRMP and AOA match data consistently show strong DO representation in PM&R, and many residency programs value the whole-person perspective osteopathic training provides.
The Medical School Timeline: Preclinical and Clinical Training
The first two years are preclinical, covering foundational sciences such as anatomy, physiology, pharmacology, and pathology. Instruction blends lectures, labs, and early clinical exposure. In years three and four, students rotate through core specialties: internal medicine, surgery, pediatrics, psychiatry, and others. Aspiring physiatrists should arrange elective rotations in PM&R during the third or fourth year to gain hands-on experience, build relationships with faculty, and secure strong letters of recommendation.
The Financial Commitment: Understanding Medical School Debt
Medical school is a substantial investment. According to the AAMC, the median debt for 2024 graduates was $205,000, rising to $230,000 for private-school attendees and easing to $200,000 at public institutions.1 About 71% of students graduate with education debt.1 Loan repayment programs and Public Service Loan Forgiveness may reduce the burden, especially for those who pursue careers in underserved or rehabilitation settings.
Alternative Paths: IMGs and Nontraditional Students
International medical graduates must obtain ECFMG certification before applying to U.S. residencies, a process that includes passing the required USMLE exams and often demonstrating U.S. clinical experience. Match rates for IMGs in PM&R tend to be lower than for U.S. graduates, but targeted sub-internships and networking can strengthen an application. Nontraditional students, including career-changers, follow the same core steps but should emphasize resilience and relevant life experience in their personal statements and interviews.
Step 3: Pass USMLE or COMLEX Licensing Exams
MD and DO students follow parallel but distinct licensing paths, and understanding the differences matters for how you plan the final stretch before residency applications.
Two Tracks, One Goal
MD students sit for the United States Medical Licensing Examination, a three-step series administered by the NBME and FSMB. DO students take the COMLEX-USA series instead, which covers equivalent ground through an osteopathic lens. Many DO candidates also choose to take the USMLE, since some residency programs historically prefer or require it, though PM&R programs generally accept either credential.
The Step Sequence
- Step 1 (USMLE) / Level 1 (COMLEX): Taken during or after the second year of medical school. As of 2022, USMLE Step 1 converted to a pass/fail score, removing the three-digit number that once drove early residency screening.
- Step 2 CK (USMLE) / Level 2-CE (COMLEX): Completed before residency applications go out, typically in the fourth year. This is now the primary numeric benchmark programs use.
- Step 3 (USMLE) / Level 3 (COMLEX): Taken during residency. Passing it is required for full, unrestricted medical licensure in all U.S. states.
Why Step 2 CK Carries More Weight Now
With Step 1 scored pass/fail, PM&R program directors have shifted their attention to Step 2 CK scores when comparing applicants on paper. According to recent Charting Outcomes in the Match data, competitive PM&R applicants typically score in the 240 range or above on Step 2 CK. That does not mean lower scores disqualify you, but scores below that threshold can narrow your program list and require stronger letters, research, or clinical evaluations to offset.
Failure on any step has real consequences. It delays your application timeline, flags your file during residency screening, and can push your match date back by a full year. Low scores, even passing ones, carry their own costs if they fall noticeably below a program's typical range.
The practical advice is straightforward: treat Step 2 CK preparation with the same intensity that earlier cohorts brought to Step 1. Schedule dedicated study blocks, use question banks early, and give yourself enough time to retake if needed without disrupting your application cycle.
Step 4: Complete a PM&R Residency: Match Data and What to Expect
A PM&R residency trains you to become a physiatrist, specializing in physical medicine and rehabilitation. This four-year program focuses on restoring function for patients with musculoskeletal, neurological, and other disabling conditions. The residency matching process is competitive and numbers-driven, so understanding the landscape helps you prepare.
The Match Process in Context
All residency applicants enter the National Resident Matching Program (NRMP) Main Residency Match. In 2026, the match placed over 44,000 applicants into residency positions nationally, with an overall fill rate of 93.5 percent.1 For physiatry-specific data, the NRMP releases detailed tables showing positions offered, fill rates, and match outcomes by specialty. Visit nrmp.org and download the latest "Main Residency Match Results and Data" report to see how PM&R compares.
Competitiveness and Test Scores
PM&R continues to attract strong candidates. The NRMP's "Charting Outcomes in the Match" breaks down average USMLE Step 2 CK scores for matched applicants by specialty and applicant type. While aggregate data shows U.S. MD seniors had a 93.5 percent match rate across all specialties in 2026, individual specialties like PM&R often diverge.2 U.S. DO seniors matched at 93.2 percent, while U.S. citizen IMGs matched at 70.0 percent and non-U.S. citizen IMGs at 56.4 percent.2 Use the NRMP report to benchmark your own Step 2 CK score against recent cohorts and gauge where you stand.
Fellowship Pathways After Residency
Many physiatrists pursue fellowship subspecialty training. The NRMP's Specialties Matching Service coordinates a large share of these positions. In 2026, that service offered over 15,000 fellowship spots across 81 subspecialties, with an 84.4 percent fill rate.3 For PM&R-specific fellowships (brain injury, sports medicine, pain medicine, spinal cord injury, and more), the SF Match manages a separate process at sfmatch.org. The American Academy of Physical Medicine and Rehabilitation (AAPM&R) also maintains a directory of accredited programs. Both resources clarify application timelines and position numbers.
Employment Outlook and Next Steps
The demand for physiatrists remains strong, driven by an aging population and increased focus on functional outcomes. The Bureau of Labor Statistics projects continued growth for physicians and surgeons, though physiatrist-specific projections are best explored directly at bls.gov. Once you match, your residency curriculum integrates clinical rotations, research opportunities, and board exam preparation, all building toward board certification and independent practice.
PM&R residency programs consistently fill at high rates, often exceeding 95% according to the NRMP's annual Match data, reflecting strong applicant interest and solid career prospects. The AAPM&R has published workforce studies projecting a growing demand for physiatrists as the U.S. population ages and chronic conditions requiring rehabilitation services increase.
Step 5: Obtain Board Certification in PM&R
Completing your residency gets you to the finish line of training, but board certification is what signals to employers, hospitals, and patients that you have met a rigorous, peer-validated standard of competence. Technically, certification from the American Board of Physical Medicine and Rehabilitation (ABPMR) is not a legal requirement to practice, yet virtually every hospital system, rehabilitation center, and academic program treats it as a baseline expectation.
The ABPMR Certification Process
After finishing an accredited PM&R residency, physicians become eligible to sit for the ABPMR examination. The process involves two components:
- Part 1: A computer-based written examination covering the full scope of physical medicine and rehabilitation, taken after residency.
- Part 2: A clinical skills examination that assesses patient evaluation, interpretation of diagnostic studies, and treatment planning.
Candidates must pass both parts to earn initial certification. The sequence is straightforward, and most physiatrists complete both within one to two years of finishing residency.
Osteopathic Certification
DO graduates historically pursued certification through the American Osteopathic Board of Physical and Rehabilitation Medicine (AOBPMR). Since the transition to a single graduate medical education accreditation system, DO graduates completing ACGME-accredited PM&R residencies now pursue ABPMR certification through the same pathway as MD graduates. Both routes lead to the same recognized credential.
Maintenance of Certification
Board certification is not a one-time achievement. The ABPMR operates on a 10-year recertification cycle. Diplomates complete continuing medical education requirements, self-assessment modules, and a recertification examination within each cycle. The workload is spread over a decade, making it manageable alongside a full clinical schedule. Think of it as structured professional development rather than a recurring hurdle.
Subspecialty Certifications
For physiatrists who want to deepen expertise in a specific area, the ABPMR offers subspecialty certificates in several fields:
- Brain injury medicine
- Hospice and palliative care
- Neuromuscular medicine
- Pain medicine
- Pediatric rehabilitation medicine
- Spinal cord injury medicine
- Sports medicine
Each subspecialty requires additional focused training (typically a fellowship) and a separate examination. Earning one of these credentials can open doors to specialized practice settings, academic appointments, and in many cases, higher compensation.
Physiatrist Salary and Job Outlook
Physiatrists command strong compensation that reflects the length and rigor of their training. Earnings vary meaningfully by practice setting, subspecialty focus, and years in practice, with pain medicine and sports medicine subspecialists typically earning toward the higher end of the range. The broader physician workforce is projected to grow steadily through the next decade, and PM&R specialists remain in consistent demand as the population ages.

Physiatrist Salary by Subspecialty and Setting
Compensation in physical medicine and rehabilitation varies more by procedural intensity and payer mix than by almost any other specialty characteristic. Pain medicine and interventional spine physiatrists consistently command the highest salaries, often exceeding those of general PM&R physicians by $150,000 or more annually, while academic and Veterans Affairs positions trade lower base compensation for loan-forgiveness eligibility, predictable schedules, and protected teaching or research time.
Salary Ranges by Subspecialty and Setting (2025)
The table below summarizes recent compensation data across common PM&R subspecialties and employment models:1
| Subspecialty / Setting | Typical Salary Range |
|---|---|
| Pain Medicine , Private Practice | $500,000, $800,000 |
| Pain Medicine , Hospital-Employed | $425,000, $550,000 |
| Sports Medicine , Private Practice | $400,000, $550,000 |
| Sports Medicine , Academic Medical Center | $300,000, $375,000 |
| Spinal Cord Injury , Hospital-Employed | $340,000, $410,000 |
| Brain Injury , VA | $280,000, $340,000 |
| General PM&R , Academic Medical Center | $280,000, $360,000 |
| Pediatric Rehabilitation , Hospital-Employed | $300,000, $360,000 |
The national average salary for physiatrists stands at approximately $365,500 (2024 to 2025), placing PM&R squarely in the middle tier of physician compensation.1 According to the American Academy of Physical Medicine and Rehabilitation, private-practice physiatrists who perform high volumes of interventional procedures (epidural injections, radiofrequency ablation, trigger-point injections) often earn $400,000 to $650,000 annually, driven by procedural revenue and the ability to manage their own payer mix.2
Why Pain Medicine and Interventional Spine Lead
Physiatrists who subspecialize in pain management or interventional spine generate significantly higher revenue per clinical hour because procedures carry higher relative value units (RVUs) than evaluation-and-management visits alone. Many practices also operate ambulatory surgery centers or procedure suites, creating additional income streams. These roles often require longer training (a one-year pain fellowship after PM&R residency) and higher patient volumes, but the financial return is substantial.
Academic and VA Trade-Offs
Academic medical centers and Veterans Affairs hospitals typically offer salaries $75,000 to $150,000 below private-practice benchmarks. In exchange, these positions frequently qualify for Public Service Loan Forgiveness after ten years of payments, provide structured teaching and research opportunities, and offer more predictable call schedules. For early-career physiatrists carrying $200,000 or more in federal student loans, the effective value of PSLF can rival or exceed the nominal salary gap.
Physiatrist vs. Orthopedist vs. Related Careers
Physiatrists, orthopedic surgeons, neurologists, and physical therapists all work to improve patient function and quality of life, but their education paths, daily responsibilities, and salary structures vary considerably. Understanding these differences helps prospective clinicians choose the career that best matches their interests and goals.
Training and Education Comparison
All physician paths (physiatrist, orthopedic surgeon, neurologist) begin with a four-year bachelor's degree, four years of medical school (MD or DO), and then a residency. Physical therapists earn a Doctor of Physical Therapy (DPT), which typically takes three years after a bachelor's degree, with no medical school required.
- Physiatrist (PM&R): Four-year residency in physical medicine and rehabilitation, often including one year of internal medicine or transitional training. Total post-bachelor training: 8 years.
- Orthopedic surgeon: Five-year residency in orthopedic surgery, typically including a general surgery internship. Total: 9 years.
- Neurologist: Four-year residency in neurology, with a preliminary year in internal medicine. Total: 8 years.
- Physical therapist: Three-year DPT program. Total post-bachelor training: 3 years.
Residency program lengths are set by the Accreditation Council for Graduate Medical Education (ACGME) for physicians and by the Commission on Accreditation in Physical Therapy Education (CAPTE) for DPT programs.
Scope of Practice and Conditions Treated
Each profession focuses on a distinct set of conditions and interventions:
- Orthopedic surgeons are surgical specialists who manage musculoskeletal injuries and diseases. They perform procedures like joint replacements, fracture repairs, and arthroscopic surgery. Common conditions include osteoarthritis, torn ligaments, and spinal deformities.
- Neurologists diagnose and treat disorders of the nervous system without surgery. They manage conditions such as epilepsy, multiple sclerosis, stroke, and migraine. Advanced training in neurophysiology or movement disorders may further refine their focus.
- Physiatrists (also called PM&R physicians) are non-surgical specialists who design comprehensive rehabilitation plans. They treat patients with spinal cord injuries, traumatic brain injuries, amputation, and chronic pain. Their goal is to restore maximum function, often coordinating with physical and occupational therapists.
- Physical therapists work directly with patients to improve mobility, reduce pain, and prevent disability through exercise, manual therapy, and education. They carry out the treatment plan under the guidance of a referring physician or independently, depending on state direct access laws.
Salary Comparison
Earnings reflect the length of training and surgical involvement. The Bureau of Labor Statistics (BLS) Occupational Employment and Wage Statistics for May 2024 provide national median annual wages for these occupations. For physiatrists, the BLS does not have a specific code; however, data from the American Academy of Physical Medicine and Rehabilitation (AAPM&R) offers a more targeted figure.
- Orthopedic surgeons, except pediatric (SOC 29-1242): $378,250
- Neurologists (SOC 29-1217): $267,660
- Physical therapists (SOC 29-1123): $97,720
- Physiatrists (classified under Physicians, All Other, SOC 29-1131): BLS reports $236,000 for the broader group. The AAPM&R 2024 Compensation Survey reports a median salary of $306,000 for physiatrists.
These are national estimates; salaries vary by region, practice setting, and years of experience.
Choosing Your Path
If you are drawn to hands-on surgery and treating acute injuries, orthopedic surgery may be the right fit. Those fascinated by the brain and nervous system disorders may lean toward neurology. Physiatry is ideal for clinicians who want to lead rehabilitation and manage chronic disability without surgery, while physical therapy suits those who prefer close patient contact through movement and exercise. Exploring professional organizations like the AAPM&R, American Academy of Orthopaedic Surgeons (AAOS), American Academy of Neurology (AAN), and American Physical Therapy Association (APTA) can provide deeper insight into each career.
The financial commitment to physiatry is substantial, with medical school debt commonly reaching $200,000 to $300,000, but the return on investment is strong for those with patience: a median physician salary exceeding $250,000, combined with access to Public Service Loan Forgiveness for those practicing in academic medical centers or VA hospitals, can make the 12-plus years of training well worth the wait.
Frequently Asked Questions About Becoming a Physiatrist
These are some of the most common questions prospective physiatrists ask when mapping out their training path. Each answer draws on the data and timelines covered throughout this guide.
Related Psychology Careers
- BCBA
- Biogerontologist
- Child Psychologist
- Clinical Psychologist
- Cognitive Neuroscientist
- Cognitive Psychologist
- Comparative Psychologist
- Consumer Psychologist
- Counseling Psychologist
- Criminal Psychologist
- Cultural Psychologist
- Forensic Psychologist
- Gerontologist
- Geropsychologist
- Health Psychologist
- Media Psychologist
- Military Psychologist
- Navy Psychologist
- Neurologist
- Neuropsychologist
Show 20 more
- Personnel Psychologist
- Police Psychologist
- Positive Psychologist
- Psychiatrist
- Psychological Anthropologist
- Psychometrician
- Rehabilitation Psychologist
- School Psychologist
- Social Psychologist
- Spiritual Psychologist
- Sports Psychologist
- Transpersonal Psychologist
- Air Force Psychologist
- Applied Psychologist
- Army Psychologist
- Educational Psychologist
- Engineering Psychologist
- Environmental Psychologist
- Experimental Psychologist
- Industrial-Organizational Psychologist